Modern occupational hygiene practices help reduce cases of phosphorus necrosis of the jaw

By Maria Perno Goldie, RDH, MS
One of the workshop sessions was “Emerging Science That Influences Practice.” One of the presenters of that workshop was Philippe Hujoel, PhD, DDS, MSD, MS. Dr. Hujoel has a DDS from the University of Brussels, Belgium, an MSD and a PhD in epidemiology from the University of Washington, and an MS in biostatistics from the University of Michigan. He is a Professor, Oral Health Sciences, and Adjunct Professor, Epidemiology, at the University of Washington. He also maintains a private practice in Shoreline, WA. His research interests include: etiology and treatment of oral and craniofacial diseases; outcomes assessment of periodontal therapy; and the role of nutrition in dentistry Dr. Hujoel has over 100 publications in peer-reviewed journals and has authored several book chapters on epidemiology and periodontics. The recipient of numerous awards, he has served on the editorial boards of several dental journals and has given dozens of scientific presentations at sites around the world. This article is a synopsis of the workshop.Dr. Hujoel reviewed the risk of bisphosphonate-induced osteonecrosis of the jaws based on new findings from several large studies, including data from the NIDCR-funded trans-dental practice-based research networks (CONDOR) studies.(1,2)
One of the workshop sessions was “Emerging Science That Influences Practice.” One of the presenters of that workshop was Philippe Hujoel, PhD, DDS, MSD, MS. Dr. Hujoel has a DDS from the University of Brussels, Belgium, an MSD and a PhD in epidemiology from the University of Washington, and an MS in biostatistics from the University of Michigan. He is a Professor, Oral Health Sciences, and Adjunct Professor, Epidemiology, at the University of Washington. He also maintains a private practice in Shoreline, WA. His research interests include: etiology and treatment of oral and craniofacial diseases; outcomes assessment of periodontal therapy; and the role of nutrition in dentistry Dr. Hujoel has over 100 publications in peer-reviewed journals and has authored several book chapters on epidemiology and periodontics. The recipient of numerous awards, he has served on the editorial boards of several dental journals and has given dozens of scientific presentations at sites around the world. This article is a synopsis of the workshop.Dr. Hujoel reviewed the risk of bisphosphonate-induced osteonecrosis of the jaws based on new findings from several large studies, including data from the NIDCR-funded trans-dental practice-based research networks (CONDOR) studies.(1,2)

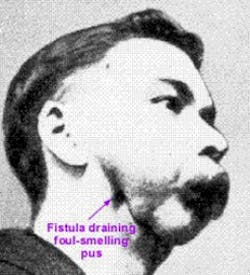
He began by explaining “Phossy jaw”, formally phosphorus necrosis of the jaw. It is described as an occupational disease of those who work with white phosphorus, also known as yellow phosphorus, without proper safeguards. It was most commonly seen in workers in the match industry in the 19th and early 20th century. Modern occupational hygiene practices have eliminated the working conditions which caused this disease.Links to bisphosphonates
A related condition, bisphosphonate-associated osteonecrosis of the jaw (BON), has been described as a side-effect of amino-bisphosphonates, a class of phosphorus-based drugs that inhibit bone resorption, and are used widely for treating osteoporosis, bone disease in cancer and some other conditions.(3) BON is primarily associated with the use of intravenous bisphosphonates in the treatment of cancer. The percentage incidence of BON from this use is approximately 1,000 times higher than the incidence of BON caused by the use of oral bisphosphonates.(4)
A related condition, bisphosphonate-associated osteonecrosis of the jaw (BON), has been described as a side-effect of amino-bisphosphonates, a class of phosphorus-based drugs that inhibit bone resorption, and are used widely for treating osteoporosis, bone disease in cancer and some other conditions.(3) BON is primarily associated with the use of intravenous bisphosphonates in the treatment of cancer. The percentage incidence of BON from this use is approximately 1,000 times higher than the incidence of BON caused by the use of oral bisphosphonates.(4)

Case reports and cohort studies have linked bisphosphonate therapy and osteonecrosis of the jaws (ONJ), but neither causality nor specific risks for lesion development have been clearly established. The CONDOR Collaborative Group conducted a 1:3 case-control study with three dental Practice-based Research Networks, using dentist questionnaires and patient interviews for collection of data on bisphosphonate therapy, demographics, co-morbidities, and dental and medical treatments.(2) They enrolled 191 ONJ cases and 573 controls in 119 dental practices. Bisphosphonate use was strongly associated with ONJ (odds ratios [OR] 299.5 {95%CI 70.0-1282.7} for intravenous [IV] use and OR = 12.2 {4.3-35.0} for oral use). Risk markers included local suppuration (OR = 7.8 {1.8-34.1}), dental extraction (OR = 7.6 {2.4-24.7}), and radiation therapy (OR = 24.1 {4.9-118.4}). When cancer patients (n = 143) were excluded, bisphosphonate use (OR = 7.2 {2.1-24.7}), suppuration (OR = 11.9 {2.0-69.5}), and extractions (OR = 6.6 {1.6-26.6}) remained associated with ONJ. Higher risk of ONJ began within 2 years of bisphosphonate initiation and increased four-fold after 2 years. Both IV and oral bisphosphonate use were strongly associated with ONJ. Duration of treatment > 2 years; suppuration and dental extractions were independent risk factors for ONJ.(2) As with any study, this one had strengths and limitations. One limitation is the fact that information about medication use was obtained from telephone interviews. Though patients were asked in a pre-interview mailing to help the process by listing all their past and current drugs prior to the call, this method is still subject to recall bias. A strength of the study is that it was conducted in community-based dental practices spanning the US rather than at academic medical centers. According to the authors, this increases the probability that the participants were more typical of the general population and strengthening generalizability.(2) The conclusion of this case-control study supports a causal link between bisphosphonates and ONJ. The highest risk was found for patients receiving more potent bisphosphonates, but substantial associations existed for oral-bisphosphonate-treated, noncancer patients, as well.(2)Since the North American Dental Hygiene Research Conference a few weeks ago, a new paper has been published by the American Dental Association (ADA). This paper is an executive summary based on a report developed by an advisory committee of the American Dental Association Council on Scientific Affairs.(5) They assessed the literature by means of a systematic search.(5) The authors searched MEDLINE for literature published between May 2008 (the end date of the last search) and February 2011. The purpose of the report is to help clinicians make treatment decisions based on the current best evidence, and an expert opinion when necessary, for patients being treated with antiresorptive agents. There is a table (Table 1) in the paper listing the various antoresprptive medications.(6) It lists the brand name, generic name, dosage, the manufacturer, the date it was approved, and indications for each drug. The advisory committee assembled the report as an educational tool to assist clinicians when discussing this subject with patients, and in the treatment of those taking antiresorptive therapy. It focuses on patients receiving antiresorptive therapy for low bone mass rather than on patients receiving antiresorptive therapy for cancer treatment, as patients with low bone mass are seen routinely in dental offices. This report updates the 2008 advisory statement from the American Dental Association Council on Scientific Affairs.(7) The report contains recommendations based on the findings of the literature search and on expert opinion that relate to general dentistry; periodontal disease management; implant placement and maintenance; oral and maxillofacial surgery; endodontics; restorative dentistry and prosthodontics; orthodontics; and C-terminal telopeptide testing and drug holidays. The conclusions are that the highest reliable estimate of antiresorptive agent–induced osteonecrosis of the jaw (ARONJ) prevalence is approximately 0.10 percent.(8) Osteoporosis is responsible for considerable morbidity and mortality. Consequently the benefit provided by antiresorptive therapy outweighs the low risk of developing osteonecrosis of the jaw. A preventive oral health program consisting of good oral hygiene practices and regular oral care may be the optimal approach for lowering ARONJ risk. No validated diagnostic technique exists to determine which patients are at increased risk of developing ARONJ. Discontinuing bisphosphonate therapy may not lower the risk but may have a negative effect on low-bone-mass–treatment outcomes.(5)Other items discussed in the report are C-terminal telopeptide testing and drug holidays. Serum-based bone turnover markers are biochemical markers of bone remodeling. Two such markers are C-terminal telopeptide (CTX) and N-terminal telopeptide.(5) Researchers in some studies have promoted the use of serum CTX to predict the risk of developing ARONJ, while others have questioned its utility.(9,10) As well, there is insufficient evidence to recommend a holiday from antiresorptive drug therapy or waiting periods before performing dental treatment for prevention of ARONJ.(5)When treating patients in our offices, we need to perform a complete medical and dental history, and full risk assessment. If patients are taking bisphosphonates for any reason, we need to educate them about the possible side effects, and how the drugs may affect the oral cavity. A new patient handout is available, and the print version of the page may be clipped and photocopied as a handout for patients without reprint permission from the ADA Publishing.(11) “For the Dental Patient” provides general information on dental treatments to patients. It is designed to initiate discussion between the oral health care provider and patient about treatment options and does not substitute for professional assessment based on the individual patient’s needs and desires. Any other use, copying or distribution of the material, whether in printed or electronic form and including the copying and posting of this material on a Web site, is strictly prohibited without prior written consent of the ADA Publishing Division.

Judith Huff-Shack, RDH, BS, also spoke about Emerging Science That Influences Practice. Judith discussed tobacco cessation and a website designed to help providers help smokers and users of tobacco. She told us about Refer-a-Smoker, an interactive website to assist medical providers in helping their patients quit smoking.(12) For questions from medical providers about the website or project, contact Kathryn at [email protected] or 508-856-3547. For questions from dental providers about the website or project, contact Jessica at [email protected] or 205-996-4957. The project was funded by the National Cancer Institute (NCI) and the National Institute of Dental and Craniofacial Research (NIDCR) at the National Institutes of Health (NIH).References
1. Hujoel P for the CONDOR Collaborative Group. Bisphosphonate-related osteonecrosis of the jaws. Second North American Conference on Dental Hygiene Research. October 20-22, 2011. Bethesda, Maryland.2. Research Reports - Clinical: Barasch A, Cunha-Cruz J, Curro FA, Hujoel P, Sung AH, Vena D, Voinea-Griffin AE, and the CONDOR Collaborative Group. Risk Factors for Osteonecrosis of the Jaws: a Case-Control Study from the CONDOR Dental PBRN J Dent Res April 2011 90: 439-444, first published on February 11, 2011 doi:10.1177/0022034510397196.3. Durie BG, Katz M, Crowley J (July 2005). "Osteonecrosis of the jaw and bisphosphonates". N. Engl. J. Med. 353 (1): 99–102; discussion 99–102.4. Cartsos VM, Zhu S, Zavras AI (January 2008). "Bisphosphonate use and the risk of adverse jaw outcomes: a medical claims study of 714,217 people". J Am Dent Assoc 139 (1): 23–30.5. Hellstein JW, Adler RA, Edwards B, Jacobsen PL, Kalmar JR, Koka S, Migliorati CA, Ristic H, for the American Dental Association Council on Scientific Affairs Expert Panel on Antiresorptive Agents. Managing the care of patients receiving antiresorptive therapy for prevention and treatment of osteoporosis. Executive summary of recommendations from the American Dental Association Council on Scientific Affairs. The Journal of the American Dental Association November 1, 2011 vol. 142 no. 11 1243-1251. www.ada.org/sections/professionalResources/pdfs/topics_aronj_report.pdf. Accessed Nov. 7, 2011. 6. Landesberg R, Eisig S, Fennoy I, Siris E. Alternative indications for bisphosphonate therapy. J Oral Maxillofac Surg 2009;67(5 suppl): 27-34.7. Edwards BJ, Hellstein JW, Jacobsen PL, Kaltman S, Mariotti A, Migliorati CA; American Dental Association Council on Scientific Affairs Expert Panel on Bisphosphonate-Associated Osteonecrosis of the Jaw. Updated recommendations for managing the care of patients receiving oral bisphosphonate therapy: an advisory statement from the American Dental Association Council on Scientific Affairs (published correction appears in JADA 2009;140[5]:522). JADA 2008;139(12):1674-1677.8. Lo JC, O’Ryan FS, Gordon NP, et al; Predicting Risk of Osteonecrosis of the Jaw with Oral Bisphosphonate Exposure (PROBE) Investigators. Prevalence of osteonecrosis of the jaw in patients with oral bisphosphonate exposure. J Oral Maxillofac Surg, 2010;68(2):243-253.9. Lazarovici TS, Mesilaty-Gross S, Vered I, et al. Serologic bone markers for predicting development of osteonecrosis of the jaw in patients receiving bisphosphonates. J Oral Maxillofac Surg, 2010;68(9):2241-2247.10. Lee CY, Suzuki JB. CTX biochemical marker of bone metabolism: is it a reliable predictor of bisphosphonate-associated osteonecrosis of the jaws after surgery? Part II: a prospective clinical study. Implant Dent 2010;19(1):29-38.11. American Dental Association (ADA) Division of Science. For the Dental Patient. Osteoporosis medications and your dental health. The Journal of the American Dental Association November 1, 2011 vol. 142 no. 11 1320.12. referasmoker.org/. Additional reading
1. National Osteoporosis Foundation. Bone health basics: why bone health is important. www.nof.org/aboutosteoporosis/bonebasics/whybonehealth. Accessed Nov. 7, 2011.2. Bauer DC, Black DM, Garnero P, et al. Change in bone turnover and hip, non-spine, and vertebral fracture in alendronate-treated women: the fracture intervention trial. J Bone Miner Res 2004;19(8): 1250-1258.3. Silverman SL, Watts NB, Delmas PD, Lange JL, Lindsay R. Effectiveness of bisphosphonates on nonvertebral and hip fractures in the first year of therapy: the risedronate and alendronate (REAL) cohort study. Osteoporos Int 2007;18(1):25-34.4. McClung MR, Geusens P, Miller PD, et al. Effect of risedronate on the risk of hip fracture in elderly women. Hip Intervention Program Study Group. N Engl J Med 2001;344(5):333-340.5. Kurtzman GM, Silverstein LH, Peden J, and Shatz PC. Implications of bisphosphonate use for the dentist. Implant Dentistry Today. February 2007 Volume 1 Number1, pp.24-33.6. Goldie MP. Bisphosphonate use and osteonecrosis of the jaw: association or risk based on evidence? ACCESS, 2009.7. Task Force on Bisphosphonate-Related Osteonecrosis of the Jaws: American Association of Oral and Maxillofacial Surgeons Position Paper on Bisphosphonate-Related Osteonecrosis of the Jaw—2009 Update. www.aaoms.org/docs/position_papers/bronj_update.pdf. Accessed Nov. 7, 2011.
1. Hujoel P for the CONDOR Collaborative Group. Bisphosphonate-related osteonecrosis of the jaws. Second North American Conference on Dental Hygiene Research. October 20-22, 2011. Bethesda, Maryland.2. Research Reports - Clinical: Barasch A, Cunha-Cruz J, Curro FA, Hujoel P, Sung AH, Vena D, Voinea-Griffin AE, and the CONDOR Collaborative Group. Risk Factors for Osteonecrosis of the Jaws: a Case-Control Study from the CONDOR Dental PBRN J Dent Res April 2011 90: 439-444, first published on February 11, 2011 doi:10.1177/0022034510397196.3. Durie BG, Katz M, Crowley J (July 2005). "Osteonecrosis of the jaw and bisphosphonates". N. Engl. J. Med. 353 (1): 99–102; discussion 99–102.4. Cartsos VM, Zhu S, Zavras AI (January 2008). "Bisphosphonate use and the risk of adverse jaw outcomes: a medical claims study of 714,217 people". J Am Dent Assoc 139 (1): 23–30.5. Hellstein JW, Adler RA, Edwards B, Jacobsen PL, Kalmar JR, Koka S, Migliorati CA, Ristic H, for the American Dental Association Council on Scientific Affairs Expert Panel on Antiresorptive Agents. Managing the care of patients receiving antiresorptive therapy for prevention and treatment of osteoporosis. Executive summary of recommendations from the American Dental Association Council on Scientific Affairs. The Journal of the American Dental Association November 1, 2011 vol. 142 no. 11 1243-1251. www.ada.org/sections/professionalResources/pdfs/topics_aronj_report.pdf. Accessed Nov. 7, 2011. 6. Landesberg R, Eisig S, Fennoy I, Siris E. Alternative indications for bisphosphonate therapy. J Oral Maxillofac Surg 2009;67(5 suppl): 27-34.7. Edwards BJ, Hellstein JW, Jacobsen PL, Kaltman S, Mariotti A, Migliorati CA; American Dental Association Council on Scientific Affairs Expert Panel on Bisphosphonate-Associated Osteonecrosis of the Jaw. Updated recommendations for managing the care of patients receiving oral bisphosphonate therapy: an advisory statement from the American Dental Association Council on Scientific Affairs (published correction appears in JADA 2009;140[5]:522). JADA 2008;139(12):1674-1677.8. Lo JC, O’Ryan FS, Gordon NP, et al; Predicting Risk of Osteonecrosis of the Jaw with Oral Bisphosphonate Exposure (PROBE) Investigators. Prevalence of osteonecrosis of the jaw in patients with oral bisphosphonate exposure. J Oral Maxillofac Surg, 2010;68(2):243-253.9. Lazarovici TS, Mesilaty-Gross S, Vered I, et al. Serologic bone markers for predicting development of osteonecrosis of the jaw in patients receiving bisphosphonates. J Oral Maxillofac Surg, 2010;68(9):2241-2247.10. Lee CY, Suzuki JB. CTX biochemical marker of bone metabolism: is it a reliable predictor of bisphosphonate-associated osteonecrosis of the jaws after surgery? Part II: a prospective clinical study. Implant Dent 2010;19(1):29-38.11. American Dental Association (ADA) Division of Science. For the Dental Patient. Osteoporosis medications and your dental health. The Journal of the American Dental Association November 1, 2011 vol. 142 no. 11 1320.12. referasmoker.org/. Additional reading
1. National Osteoporosis Foundation. Bone health basics: why bone health is important. www.nof.org/aboutosteoporosis/bonebasics/whybonehealth. Accessed Nov. 7, 2011.2. Bauer DC, Black DM, Garnero P, et al. Change in bone turnover and hip, non-spine, and vertebral fracture in alendronate-treated women: the fracture intervention trial. J Bone Miner Res 2004;19(8): 1250-1258.3. Silverman SL, Watts NB, Delmas PD, Lange JL, Lindsay R. Effectiveness of bisphosphonates on nonvertebral and hip fractures in the first year of therapy: the risedronate and alendronate (REAL) cohort study. Osteoporos Int 2007;18(1):25-34.4. McClung MR, Geusens P, Miller PD, et al. Effect of risedronate on the risk of hip fracture in elderly women. Hip Intervention Program Study Group. N Engl J Med 2001;344(5):333-340.5. Kurtzman GM, Silverstein LH, Peden J, and Shatz PC. Implications of bisphosphonate use for the dentist. Implant Dentistry Today. February 2007 Volume 1 Number1, pp.24-33.6. Goldie MP. Bisphosphonate use and osteonecrosis of the jaw: association or risk based on evidence? ACCESS, 2009.7. Task Force on Bisphosphonate-Related Osteonecrosis of the Jaws: American Association of Oral and Maxillofacial Surgeons Position Paper on Bisphosphonate-Related Osteonecrosis of the Jaw—2009 Update. www.aaoms.org/docs/position_papers/bronj_update.pdf. Accessed Nov. 7, 2011.

Maria Perno Goldie, RDH, MS
To read previous articles in RDH eVillage FOCUS from 2011 written by Maria Perno Goldie, go to articles.