October is Breast Cancer Awareness Month

One of the simplest and most important things to know about the risk for breast cancer is to know one’s family history. Breast cancer risk is higher among women whose close blood relatives have had the disease. This is true whether or not you, or they, have the “breast cancer gene” (BRCA 1 or BRCA 2).(1) If a person has a first-degree relative (mother, sister or daughter) with breast cancer, they are at increased risk. If they have two, first-degree relatives, the risk is even higher. If the relative was diagnosed before age 50, the risk increases. A lesser known fact is that a history of breast cancer in a male relative (father or brother) also increases risk, although the risk is smaller. Just to be clear, the increased risk is only for blood relatives, no in-laws or step relationships. The family link seems to indicate that other genes beyond BRCA1 or 2 put women at higher risk for developing the disease. These additional genes are yet to be identified. If one has close relatives with breast cancer, they are probably aware. It is a good to keep records, and to be sure the treating physician knows this important fact. You can use the Sutter Health MyLifeStages “medical family tree” as an easy way to track all diseases in your family. Download the Medical Family Tree today and complete it.(2)
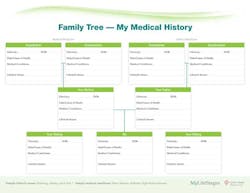
Note: If you are not signed in or not a member, you will be asked to sign in or register for free.
Should You Have Genetic Testing for Breast Cancer? The BRCA1 and BRCA2 genes belong in a class of genes known as tumor suppressors. The role of these genes is to repair cellular damage and keep cells growing normally. Changes in these genes have been linked to hereditary breast and ovarian cancer.
Both women and men can inherit a BRCA gene change (mutation) and pass it on to their children. But not everyone who inherits BRCA gene changes will get cancer. These gene changes are responsible for 5 to 10 percent of breast cancers, and 10 to 15 percent of ovarian cancers, according to the National Cancer Institute. Genetic testing for breast cancer, using a blood sample, is only recommended for those with a strong family history (parents, sisters, brothers, and children) of breast or ovarian cancer. Some ethnic and geographic populations have higher frequencies of specific BRCA1 and BRCA 2 mutations, such as in the Ashkenazi Jewish population.
Fortunately, BRCA mutations are rare, occurring in about one in 800 people. Genetic counseling, before and after a BRCA test, is very important to help understand the benefits, risks, and possible outcomes of the test. Most insurance companies will cover the cost of the genetic testing for those that meet the conditions of testing. Federal and state laws help ensure the privacy of a person’s genetic information, and provide protection against discrimination in health insurance and employment practices. If you’re in a family where there is a BRCA mutation and you don’t have the mutation, your risk of breast cancer is no greater than anyone with a family history of breast cancer. For women who have inherited a mutated BRCA gene, the chances of developing breast cancer in their lifetime however may be as high as 80 percent, according to the American Cancer Society.(3) There are several choices are available for managing cancer risks in those who have BRCA1 and BRCA2 gene mutations. However, high-quality data on the effectiveness of these options are limited. 1. Cancer screening - A way of detecting the disease early when it may be the most treatable. Breast cancer screening methods include mammography, MRI, and clinical breast exams. For ovarian cancer, methods include transvaginal ultrasound, blood tests for CA-125 antigen, and clinical exams.(4,5,6)

2. Prophylactic surgery – Removing as much of the “at risk” tissue as possible in order to reduce the chance of developing these cancers. 3. Risk avoidance – of certain behaviors that have been associated with breast and ovarian cancer in the general population. This includes: maintaining a healthy weight; staying active; eating a diet low in fat, especially saturated fats; limiting alcoholic drinks; breast feeding; giving birth by age 20; limiting exposure to hormone replacement therapy (HRT); and having a yearly professional breast examination. 4. Chemoprevention – involves the use of natural or synthetic substances to reduce the risk of developing cancer or to reduce the chance that the cancer will come back (such as Tamoxifen).(7) While the thought of gene testing may be a scary process, not knowing whether you have a BRCA gene mutation might keep you from knowing how high your risk actually may be. It could keep you from taking action that could reduce your risk of developing these diseases.Breast Cancer Treatment Regimens There are cancer treatment regimen charts based on the most recent National Comprehensive Cancer Network (NCCN) guidelines and provide physicians and patients with current information. The charts are comprehensive and easy to read, and can be a great resource for nurses, pharmacists, and physicians when deciding on the appropriate drug therapy for their cancer patients. The selection, dosing, and administration of anticancer agents and the management of associated toxicities are complex. Drug dose modifications and schedule and initiation of supportive care interventions are often necessary because of expected toxicities and because of individual patient variability, prior treatment, and comorbidities. Thus, the optimal delivery of anticancer agents requires a healthcare delivery team experienced in the use of such agents and the management of associated toxicities in patients with cancer. The cancer treatment regimens below may include both FDA-approved and unapproved uses/regimens and are provided as references only to the latest treatment strategies. Clinicians must choose and verify treatment options based on the individual patient.(8).
For more information on , see the NBCAM website. (9)References 1. http://www.cancer.gov/cancertopics/factsheet/Risk/BRCA. 2. https://www.mylifestages.org/health/senior_health/medical_family_tree.page. 3. http://www.cancer.org/Cancer/BreastCancer/DetailedGuide/breast-cancer-risk-factors. 4. https://www.mylifestages.org/health/breast/breast_cancer_screening.page?. 5. http://www.cancer.gov/cancertopics/factsheet/detection/mammograms. 6. http://www.cancer.gov/cancertopics/pdq/screening/breast/HealthProfessional. 7. https://www.mylifestages.org/health/breast/reduce_breast_cancer_risk.page. 8. http://www.chemotherapyadvisor.com/breast-cancer-treatment-regimens/article/218154/. 9. http://www.nbcam.org/.

Maria Perno Goldie, RDH, MS
To read previous RDH eVillage FOCUS articles by Maria Perno Goldie, go to articles.