Dental health professional shortage areas and inadequate preventive measures to blame for nation's poor oral health
January 11, 2013
A debate is taking place about the future of dentistry and the ability to provide care to those in need. Some reports say that there are more dentists retiring each year than there are dental school graduates to replace them; others say that there are enough dentists to provide care, but that limited access to care is to blame for our nation's poor oral health.
Because most dentists take on the burden of running their own business while paying off growing student loan debt, working in an affluent area that promises profit is more appealing than working in a low-income and Medicaid-reliant area.
South Dakota earns "D" for prevention, gives more liberty to hygienists
The U.S. isn't doing enough to prevent tooth decay, says Pew report
Starting a nationwide conversation on declining oral health
Called Health Professional Shortage Areas (HPSA) or “dental deserts,” it is these areas, not an overall shortage of dentists, that cause limited access to care, argues Dr. Robert A. Faiella, American Dental Association president.
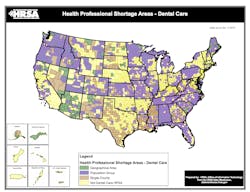
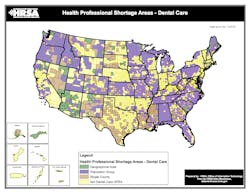
Recently, the Human Resources and Services Administration issued data on designated dental HPSAs.
HPSAs are made up of three kinds of designations: geographic area, population, or facility.
- Geographic area: Must have a doctor-to-patient ratio of at least 5,000:1*, be a logical area for a practice, and have dental professionals for the area who are too busy, far away, or inaccessible to the majority of the community.
- Population: Residents must reside in an area that would be fit to house a practice, have access barriers, and have a doctor-to-patient-ratio of 4,000:1. (Members of Federally recognized Native American tribes are automatically a designated population HPSA group.)
- Facilities: Must be a federal or state correctional facility that has more than 250 inmates with a doctor-to-patient ratio of 1,500:1 or a public or non-profit dental facility that provides care to an HPSA group but is unable to meet the needs of the community.
Currently, there are 4,595 HPSA designations with a total population of 45,086,843 people, including an estimated total underserved population to be 30,605,273.
Mississippi has the largest percentage of its population living in dental HPSAs. As of data reported January 2013 and population totals from 2011, 60% of Mississippi’s population was living in an HPSA. The next closest state is Louisiana, with 46% living in an HPSA, and third is New Mexico, at 33%.
These three states share a similar fate in the Pew report. Mississippi and Louisiana earned a “D,” while New Mexico earned a “C.” Mississippi is also one of the eight states that employs strict rules for hygienists, requiring a dentist’s exam and supervision before a hygienist can work in a school.
The five states with a low percentage (under 5%) of people living in HPSAs are:
- New Jersey: .081%
- Nebraska: .27%
- New Hampshire: 2.19%
- Oklahoma: 2.35%
- California: 4.08%
Even with a low HPSA population, all but one of these states still lag on preventive care, such as the use of dental sealants. Only New Hampshire got a Pew grade of “A” for prevention; the rest didn’t have such luck. California (“C”), Nebraska (“D”), Oklahoma (“D”) and New Jersey (“F”) still have improvements to make.
Former Surgeon General David Satcher, after the passing of the Affordable Care Act, addressed that it was important for this country to create a conversation and for people to be comfortable with talking to their doctors. But even more importantly, the conversation needed to work to prevent health issues.
It is a widely accepted notion that we need to improve preventive measures, but for those who already have evidence of irreversible decay, we still have to work on expanding access to care. “We now have an opportunity to dramatically increase coverage,” Satcher said at a conference in 2012. “But adding dental benefits will not translate into access to care if we do not have providers in place to offer treatment.”
---
*4,000:1 if there is an unusually high need for dental services
