Impacted canines and orthodontic treatment
Depending on research, it is estimated that on average there is a 1.6% incidence of maxillary impacted canines. (1) Impactions are twice as common in females (1.17%) as in males (0.51%). (1) In patients who present with impacted maxillary canines, it is estimated that 8% of these are bilateral. (1) Reasons for impactions can be varied and are categorized as both localized and generalized. (2, 3) Bishara (1) reports that the most common reasons for canine impaction are usually localized and are the result of any one or combination of the following factors: tooth size/arch length discrepancies, prolonged retention, or early loss of the deciduous canine, abnormal position of the tooth bud, the presence of an alveolar cleft, ankylosis, cystic or neoplastic formation, dilacerations of the root, iatrogenic origin, and idiopathic condition. Irradiation, febrile diseases, and endocrine deficiencies are some of the general causes. (1)
ALSO BY DR. STACEY SIMMONS |We can't save them all: the missing endodontic diagnosis
The retention of impacted canines can present with complications, namely resorption of the roots of adjacent teeth and cystic lesions of the follicle. (4)
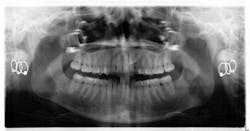
Early assessment for potential impaction is easily done by taking a panoramic radiograph at the age of 7. Ectopic positioning of canines may result in future impaction; if this is the case, then intervention can be initiated. Research has also shown that early removal of the deciduous canines can offer a favorable eruption pattern of permanent counterparts. (4,5) If crowding is present, then the arch can be expanded.
ALSO BY DR. STACEY SIMMONS | Braces: the good, the bad, and the ugly
When a full permanent dentition is present (with the exception of impacted canines), the labial/palatal position of the canine will have an influence on what the provider can do. (1) Arguably, obtaining a CBCT is considered mandatory and will allow for a more inclusive treatment plan creation. If angulation is favorable, then consideration to remove the primary canine and wait six months to see if there is movement of the permanent canine is an option. If extraction of the canine(s) is needed, then a premolar substitution, which is dependent on occlusion, can be used in the space. An implant can also be an appropriate alternative. When pulling a canine into the occlusal arch, there is risk involved. Trauma to adjacent teeth (root resorption) and ankylosis are some of the most common complications.

The patient was put in full orthodontics and referred to a surgeon for extraction of the primary canines, exposure, and placement of retention on the impacted canines to pull them directly down from their current position.


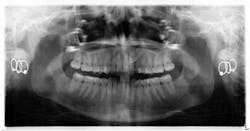
A ballista appliance was used to prevent a facial pull of the canines in order to avoid and prevent resorption of the roots of the lateral incisors. As movement progressed over the course of the next year, eruption of the canines was considered a success. Once in position, they will be pulled facially into occlusion.





The patient is pleased with the progress reached thus far and is ecstatic at the anticipation of a successful outcome.
The author would like to recognize orthodontist Padraig Dennehy, DMD, for his insight and case contribution to this write-up. He can be reached by email at [email protected].

References
1. Bishara S. Impacted maxillary canines: A review. Am J Orthod Dentofac Orthop Feb. 1992;101(2):159-171.
2. Johnston WD. Treatment of palatally impacted canine teeth. Am J Orthodon 1969;56:589-596.
3. Dachi SF, Howell FV. A survey of 3874 routine full-mouth radiographs. Oral Surg Oral Med Oral Path 1961;14:1165-1169.
4. Power SM, Short MB. An investigation into the response of palatally displaced canines to the removal of deciduous canines and an assessment of factors contributing to favorable eruption. British Journal of Orthodontics 1993;20:215-223.
5. Ericson S, Kurol J. Early treatment of palatally erupting maxillary canines by extraction of the primary canines. European Journal of Orthodontics 1988;10:283-295.
About the Author
Stacey L. Simmons, DDS
Editorial Director of DE's Breakthrough Clinical e-newsletter
Dr. Stacey Simmons grew up in Hamilton, Montana. She did part of her undergraduate work at Purdue University and then received her bachelor’s degree in exercise physiology from the University of Utah. After applying to both medical and dental school, she decided that dentistry was her career of choice. She received her DDS degree from Marquette University School of Dentistry in Milwaukee, Wisconsin, in 2004. In private practice, she focuses her care on prosthodontics and cosmetic dentistry. She is a guest lecturer in the Anatomy and Physiology Department at the University of Montana. Outside the office, she trains for triathlons and spends time with her family. You may contact Dr. Simmons by email at [email protected].
In 2015, Dr. Simmons became the editorial director of DE's Breakthrough Clinical with Stacey Simmons, DDS, an e-newsletter focused on breaking through plateaus in clinical practice. Subscription information may be found here.
Updated May 4, 2016