Implementing CAMBRA in the private practice: A clinical report


Since the introduction of caries management by risk assessment (CAMBRA) in 2007 (1), preventive products and protocols have flooded the marketplace (2). This has offered clinicians numerous selections for products and preventive practices, but it has also led to a lot of confusion in regard to choosing a system to implement in the private practice. We have tried many products and systems in my practice, and we have found that implementing CAMBRA is best accomplished in the private practice with simple recommendations that maximize patient compliance and predictable results. Keeping recommendations simple and economically reasonable has been the key to patient compliance. This case report details a high-risk patient, my preventive recommendations, and the clinical results.
RELATED | CAMBRA and caries detection technology
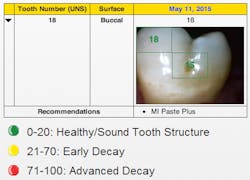
A 43-year-old male patient presented for a routine recare exam with a deep pit and staining on the buccal surface of No. 18 (figure 1). When we examined this tooth clinically, we were unsure about whether to attempt remineralization on this tooth or treat it with a small direct restoration. We decided to perform a quick scan with the Canary System by Quantum Dental Technologies. The Canary System uses a laser and heat (photothermal radiometry and modulated laser luminescence technology) to penetrate the tooth by up to 5 mm and measure the organization of the crystallization within the tooth (3). This area of concern received a Canary Score of 45. On the Canary Scale, a score of 0–20 indicates healthy tooth structure, 21–70 indicates early decay, and 71–100 indicates advanced decay (4).
We had a conversation with the patient to investigate the presence of additional risk factors that could contribute to his caries risk. The patient disclosed that he had been “stressed” and that he hadn’t been keeping up with his usual oral hygiene habits. In addition, he mentioned that he had been sipping coffee and snacking throughout the day.
The patient was classified as a high risk for the following reasons:
- Incipient caries
- Poor oral hygiene
- Diet high in sugar, carbohydrates, and acids
We informed the patient that his tooth might require a small direct restoration but also that it could be possible to remineralize the area. The patient was receptive to our remineralization protocols and consented to remineralizing the tooth and re-evaluating it during his next hygiene visit.
The following recommendations were made to minimize the patient’s caries risk:
1. Oral hygiene instructions: It was recommended that the patient resume brushing his teeth twice daily with a minimally abrasive over-the-counter toothpaste for a minimum of two minutes. The patient owned an Oral-B electric toothbrush but had not been using it. The patient agreed to use his electric toothbrushinstead of a manual toothbrush (5). Daily flossing was recommended.
2. Diet modification (6): It was recommended to discontinue sipping coffee throughout the day, consuming coffee at mealtimes instead. Additionally, it was recommended to reduce the frequency of snacks and to eat primarily during mealtimes. The snacks recommended included foods that are protein-rich, as well as caries-inhibiting, such as cheese and nuts (7).
3. Xylitol: 6–10 grams of xylitol-sweetened chewing gum per day was recommended (8). In addition, it was strongly reinforced that the patient should keep the gum out of reach of children and pets.
4. MI Paste Plus*: It was recommended that the patient apply a pea-sized amount of MI Paste Plus by GC America to his teethafter regular brushing and flossing (9,10). In addition, it was confirmed that he did not have an allergy to milk, as MI Paste Plus contains Recaldent or casein phosphopeptide-amorphous calcium phosphate (CPP-ACP).
5. Raise oral pH: To create an environment that inhibits the activity of caries-causing bacteria, it was recommended that the patient dip his toothbrush with toothpaste into baking soda before proceeding with normal brushing (11). Baking soda is water-soluble and is considered to be an extremely low abrasive.
6. MI Varnish*: The application of MI Varnish by GC America was recommended for all dental hygiene visits. Like MI Paste Plus, MI Varnish contains CPP-ACP, otherwise known as Recaldent (12). Additionally, MI Varnish has a low film thickness and is clear and esthetic. It is available in two flavors, mint and strawberry (13), and patient compliance is exceptional.
7. Re-evaluation: It was recommended that the patient return to have the tooth re-evaluated in three months.
The patient returned in three months for his hygiene visit and reported that he had been very compliant with our recommendations. He reported that he had made a significant effort in his oral hygiene practices and that he had been cognizant of his diet.
RELATED | Are you CAMBRA ready?
The clinical exam revealed a marked improvement in his oral hygiene, and a full-scan was completed with the Canary System, which revealed a Canary Score of 15—indicative of a healthy tooth structure (figure 2). We informed the patient that his tooth structure was considered healthy and that a restoration was no longer indicated. We reinforced the preventive recommendations and will monitor the patient during hygiene visits with clinical observation, interviews, and the Canary System.
The patient was pleased with this outcome, and we were satisfied that we were able to provide him with a minimally invasive approach and the optimal standard of care.
*Indicates an off-label use of the product and that the practices of the author are not consistent with the claims of the manufacturer.
References
1. Young DA, Featherstone JD. Curing the Silent Epidemic: Caries Management in the 21st Century and Beyond. J California Dental Assoc. Oct 2007;35(10):681-85.
2. Kutsch VK, et al. How to integrate CAMBRA into Private Practice. J California Dental Association. Nov 2007;35(11):778-85.
3. Jeon RJ, et al. Diagnosis of Pit and Fissure Caries Using Frequency-Domain Infrared Photothermal Radiometry and Modulated Laser Luminescence. Caries Res. 2004;38:497-513.
4. Wong B, Abrams SH, Tasevski C, Sivagurunathan K, Silvertown JD, Hellen WH, Elman G, Amaechi BT. Detection of interproximal caries in vitro using The Canary System. J Dent Res. 93(Spec Iss A):2014.
5. Yaacob M, et al. Powered versus manual toothbrushing for oral health. Cochrane Library. Published online 17 Jun 2014.
6. Moynihan PJ, Kelly SAM. Clinical Review: Effect on Caries of Restricting Sugars Intake: Systematic Review to Inform WHO Guidelines. J Dent Res. 2014;93(1):8-18.
7. Young DA, Featherstone J. Implementing Caries Risk Assessment and Clinical Interventions. Dent Clinics of North Am. July 2010;54(3):495-505.
8. Makinen KK, et al. Xylitol Chewing Gums and Caries Rates: A 40-month Cohort Study. J Dent Res. Dec 1995;74:1904-1913.
9. Robertson MA, Chung HK, English JD, Lee RP, Powers J, Nguyen JT. MI Paste Plus to prevent demineralization in orthodontic patients: A prospective randomized control trial. Am J Ortho and Dent Ortho. Nov 2011;140(5):660-668.
10. Cochrane NJ, Reynolds EC. Calcium Phosphopeptides- Mechanism of Action and Evidence for Clinical Efficacy. Adv Dent Res. 2012;24(2):41-47.
11. Cury JA, Hashizume LN, Del Bel Cury AA, Tabchoury CPM. Effect of Dentifrice Containing Fluoride and/or Baking Soda on Enamel Demineralization/Remineralization: An in-situ Study. Caries Res. 2001;35:106-110.
12. Reynolds EC. Remineralization of Enamel Subsurface Lesions by Casein Phosphopeptide-stabilized Calcium Phosphate Solutions. J Dent Res. 1997;76(9).
13. MI Varnish. GC America. http://www.gcamerica.com/products/preventive/MI_Varnish/
______________________________________________________________________________________________________________
Editor's Note: This article first appeared in Pearls for Your Practice: The Product Navigator. Click here to subscribe. Click here to submit a products article for consideration.
______________________________________________________________________________________________________________
Pamela Maragliano-Muniz, DMD, was a dental hygienist before earning her DMD from Tufts University School of Dental Medicine and her certificate in advanced prosthodontics from the UCLA School of Dentistry. She is an Associate Clinical Professor at Tufts University School of Dental Medicine and maintains a private practice in Salem, Massachusetts. Her passion for prevention has stayed with her throughout her career, and in 2010 her practice was named the Adult Preventive Care Practice of the Year by the American Dental Association.
Diane Proudy, RDH, is a dental professional whose goal is to help patients obtain and maintain optimal health—not just in terms of dentition but overall health. She graduated from Middlesex Community College with an associate's degree in dental hygiene in 2006. This is a second career for her; prior to becoming a hygienist, she worked in a manufacturing field for 20 years as a quality control inspector. She currently practices in three dental offices: Salem Dental Arts with Dr. Maragliano-Muniz, with a periodontist, and with a general dentist. She has a 21-year-old daughter, and she enjoys cooking and spending time at the beach.