Thursday Troubleshooter: Fraudulent to diagnose perio disease without full mouth probing?

QUESTION: I am a long-time RDH in California. I would appreciate any direction or information you can give me. Is it malpractice or insurance fraud if a dentist is diagnosing periodontal disease without completing a full mouth probing/charting of the patient and using limited (and poor quality) radiographs? Also, is it OK to have the RDH do the probing during the SRP appointment, after diagnosis has “been made”? This seems at the least unethical to me.
ANSWER FROM CHRISTINE TAXIN, founder of Links2Success:
The American Academy of Periodontology (AAP) Board of Trustees created a Task Force in 2014 to develop a clinical interpretation of the 1999 Classification of Periodontal Diseases and Conditions.1,2 This was done to “address concerns expressed by the education community, the American Board of Periodontology, and the practicing community that the current Classification presents challenges for the education of dental students and implementation in clinical practice.”3
There are three explicit areas of the current classification:
- Attachment level
- Chronic versus aggressive periodontitis
- Localized versus generalized periodontitis.3
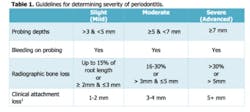
The Task Force concedes that it is sometimes difficult in clinical practice to accurately measure clinical attachment level. They suggest that a diagnosis of periodontitis should be established by using a variety of clinical and radiographic factors. These factors may include one or more sites of inflammation or bleeding on probing, radiographic bone loss, and deep probing depths or clinical attachment loss. The table below was excerpted from the new guidelines. A patient with gingival recession, no inflammation, no significant probing depths, but attachment loss, would be considered healthy. This usually occurs post-periodontal treatment.3
Read the report where I found this answer at www.perio.org/sites/.
Editor's note: This article was originally published in 2016 and has been updated as of June 2025.
References
1. Consensus Report: Chronic Periodontitis. 1999 International Workshop for a Classification of Periodontal Diseases and Conditions. Ann Periodontol 1999;4:38.
2. Eke PI, Dye BA, Wei L, Thornton-Evans GO, Genco RJ; CDC Periodontal Disease Surveillance workgroup: James Beck (University of North Carolina, Chapel Hill, USA), Gordon Douglass (Past President, American Academy of Periodontology), Roy Page (University of Washington, Seattle) Prevalence of periodontitis in adults in the United States: 2009 and 2010. J Dent Res 2012;91:914-920.
3. Eke PI, Page RC, Wei L, Thornton-Evans G, Genco RJ. Update of the case definitions for population-based surveillance of periodontitis. J Periodontol 2012;83:1449-1454.