The impact of ACA Medicaid expansion on dental visits: Study reveals mixed results

Dental coverage for adults is an optional benefit under Medicaid, one that about half of states offer. With 31 states and the District of Columbia expanding Medicaid eligibility under the Affordable Care Act (ACA), how many more low-income Americans sought dental care?
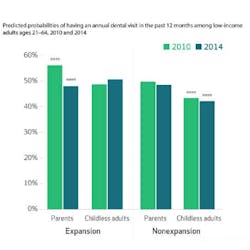
To answer this question, Astha Singhal, BDS, MPH, PhD, and her coauthors compared 2010 and 2014 data collected by the Centers for Disease Control and Prevention. Their research report is published in the April issue of Health Affairs. The study found that 1.5 million more low-income adults reported having a dental visit in 2014 than in 2010. However, among states expanding Medicaid that offer dental benefits, there was a decline in usage among adults with children, who had enjoyed this access before the ACA’s implementation (see graph).
Dr. Singhal said that these results provide evidence that the addition of new low-income patients may be straining the capacity of providers willing to treat low-income patients, and that additional policy initiatives may be needed to expand the size of this subset of the dental care delivery system.
Here is Dr. Singhal’s analysis of the study:
Study results
First of all, our study confirms that adult dental benefits under Medicaid have a significant positive impact on dental care use by low-income adults. When we examined states that provide adult dental benefits and expanded their Medicaid program under the ACA, we found that poor childless adults, a group most likely to benefit from expansion, had significantly greater dental care use after expansion. However, what is concerning is that this occurred in conjunction with a significant decline in dental care use by low-income parents in those same states.
While we did not examine supply-side issues in dental care, our results suggest that there appears to be some rate-limiting factor in terms of dental visits for low-income adults in these states. We think that after expansion, several low-income childless adults gained Medicaid dental coverage, who likely did not have prior dental coverage and hence, may have built-up dental needs. While ACA expanded coverage to millions of individuals, the dental provider capacity remained unchanged. So, now we have this group of childless adults with dental needs competing with previously enrolled low-income parents for the limited appointments with dental providers who see Medicaid patients (which has historically been a barrier to access to dental care for Medicaid enrollees).
Therefore, we recommend that expansions in coverage need to be complemented with additional policy interventions that increase the capacity of dental providers willing to treat Medicaid enrollees. These include evaluation of alternative dental provider models and increasing Medicaid reimbursement rates for dental procedures.
Future of dental care under Medicaid
Medicaid covers dental benefits for children, but dental benefits are optional for adults. The future of Medicaid and how it is administered is uncertain under various proposals and changes expected under a new administration. However, several studies show that low-income adults are one of the most vulnerable groups and face significant barriers to accessing dental care, the most important one being financial. This group is most likely to visit emergency rooms for dental problems, which is an expensive and ineffective source of seeking dental care.
Limiting federal support to Medicaid on a per-capita basis or block grants will eventually increase the pressure on states to cut costs, and adult dental care is usually one of the first benefits to be on the chopping block. Unmet dental needs can have consequences for general health and economic productivity, and it is essential that adult dental benefits not be optional under Medicaid. Also, states have several ways of investing in a population’s oral health, and future research should examine the relative merit of these policy options (expanding coverage versus increasing reimbursement versus covering more dental services etc.)
To access the report, visit HealthAffairs.org.
RELATED ARTICE:
December issue of 'Health Affairs' features divide between medical and dental care
Astha Singhal, BDS, MPH, PhD, is an assistant professor with the Department of Health Policy and Health Services Research, Boston University Henry M. Goldman School of Dental Medicine.