Group versus solo dental practices: A comparison study

The overwhelming majority of dentists continue to practice solo, despite economic pressure. Here's how those dentists compare to group practices in terms of procedures performed.
Dentists often face a decision regarding whether to practice solo or to join a group. Although there are pros and cons to both, differences between how dentists practice in solo versus in a group have not been studied extensively. With rising overhead costs and purchasing power, joining a group may seem like the smarter choice. However, according to Marc B. Cooper, DDS, almost 86% of dentists continue to practice solo despite these concerns. This article discusses trends and considerations in the differences between group and solo practices.
Sikka Software collects secure data from thousands of opt-in practices across the nation for benchmarking purposes. This article will examine data from over 12,500 opt-in dental practices, including over 2,500 group practices. Information was collected from January 2014 until July 2016 and displays monthly averages for group and solo practices. The data is HIPAA- and HITECH- compliant and is free of any identifying information. Dentists can track national trends, compare their performance, check their schedules and communicate with patients, all from their mobile phone. Download the free app for iOS and Android now or visit www.practicemobilizer.com for more information.
3–4 surface direct restorations

Surface direct restorations are not typically profitable for dentists although they are a very common procedure, including both surface amalgams and gold foil. This is why group and solo practices perform approximately the same number of these procedures each month.
3–4+ surface indirect restorations

Group practices and solo practices often accept different types of insurance plans. Group practices typically rely on HMO plans to help fill their chairs. According to Deborah Pinnock at Solstice Benefits Blog, these plans tend to be carried by lower income patients. This is because HMO plans are often less expensive and tend to pay out less. In contrast, PPO plans are accepted at solo practices that serve higher income patients.
HMO plan patients are less likely to receive a crown because the HMO margins do not make it worthwhile to perform the extra work of molding and fitting a crown. Instead, group practice dentists often stay away from crowns and prefer to use direct restorations to address their patients’ needs. Solo practices often do not have these specific limitations and are more likely to install crowns because of higher margins.
Amalgams

Due to financial constraints, group practices that accept HMOs and lower income patients are more likely to perform amalgams as opposed to the composite resin alternative. The silver fillings tend to be less cosmetically appealing but, although some patients have concerns about mercury, Colgate’s research has shown no measurable negative effects. Patients receiving these fillings typically have very few treatment options due to cost of dental care, often leaving them with amalgams as their only option.
Anterior composite

Patients with financial power or PPO plans that will help pay for composite resins are more likely to visit solo practices. Although cosmetically conscious patients often prefer anterior composites to amalgams, since silver is easily visible, this option is not financially viable for every patient. This causes the difference between the number of anterior composites performed in group as compared to solo practices.
Fixed prosthetics

HMO plans do not pay for a significant portion of a bridgework. Solo practices often accept PPOs and have patients who can financially afford the large out-of-pocket expenses associated with bridgework. In contrast, patients of HMO plans seen at group practices are more likely to receive the lower cost option of dentures. This drives the increased number of fixed prosthetics performed at solo practices over group practices.
Posterior composite
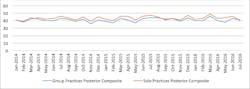
While solo practices are performing more composite fillings, group practices are not far behind. This is a sign that amalgams are decreasing in favor, as more patient prefer the cosmetic look of the composite filling.
Prophylaxis
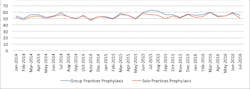
Group and solo practice are performing approximately the same number of prophylaxis cases, indicating that both groups of patients are receiving preventative oral care at the same rate. This is not unexpected, as prophylaxis is covered for patients with dental benefits.
Oral exam

Oral exams include CDT codes D0120, D0140 and D0160 (periodic oral evaluation; limited evaluation, problem focused; extensive oral evaluation, problem focused, respectively). Data indicates that solo practices are performing more oral exams, despite an equal rate of prophylaxis. This may be due to costs associated with seeing a professional for the exam as well as the prophylaxis, making oral exams costs prohibitive for some patients.
Single crowns

Single crowns are a large revenue producer for many dentists. If a patient cannot afford a crown, as might be the case with patients on HMO plans more likely to be seen by group practices, a dentist might go with a filling, a lower cost option. However, fillings are more likely to fail in these cases, and many solo practitioners with the option of accepting PPOs will not perform fillings in this circumstance, creating the disparity between solo and group practice numbers of single crowns performed.
Total direct restorations

Solo practices are doing more direct restorations overall. This may be a sign that patients with PPO plans and financial resources are more likely to be seen earlier and have problems corrected earlier before major concerns develop. This is a direct benefit of having access to dental plans, financial resources or financing options available for addressing oral health concerns.
Veneers

Veneers are a very expensive option that few patients receive and are most often not covered by benefits. In addition, many dental plans have a cap of expenses covered annually, with costs upwards of $2,000 each. Because of this, many patients in both group and solo practices cannot afford veneers, accounting for the relatively low number performed each month in the average dental practice.
Conclusion
Unfortunately for some, dental care is heavily driven by dental benefit plans, creating a two-tier system of dental care. The type of plans accepted by groups as compared to solo practices is a major driving force between the different types of procedures that these dentists perform. Financing and availability of payment options is key to providing patients the care they need for good oral health while staying in budget.
Sikka Software provides tools and services to assist dentists in evaluating their practice’s health and planning growth. Dentists can start communicating with patients securely, managing their schedule and tracking their performance on key performance indicators (KPIs), all with a free app for Apple and Android devices. Visit www.practicemobilizer.com or the Apple App or Google Play store to learn more.
For the most current dental headlines, click here.
Sources
Colgate (2014, May 12). Dental amalgam: A health risk? Colgate Oral Health Center. Retrieved from http://www.colgate.com/en/us/oc/oral-health/procedures/fillings/article/dental-amalgam-a-health-risk)
Cooper, M.B. (n.d.). 6 reasons why group dental practices may be a trend of the future. DentistryIQ. Retrieved from http://www.dentistryiq.com/articles/2012/11/6-reasons-why-group-dental-practice-may-be-a-trend-of-the-future.html
Pinnock, D. (2014, November 25). 7 differences between a dental HMO and PPO plan. Solstice Oral and Vision Health Blog. http://blog.solsticebenefits.com/solstice-member-blog/7-differences-between-a-dental-hmo-and-ppo-plan



About Sikka Software
Sikka Software provides a platform for small and medium-sized business health-care apps. The company’s products help health-care providers and other small businesses optimize their business via a series of easy to use cloud-based applications. With over 40 apps built on Sikka Platform Cloud and with over 20,030 installations, Sikka Software is the leader in the US dental, animal health, and hearing care markets. The company is now supporting a real-time optimization of its information network with providers, patients, consultants, manufacturers and financial service providers.
A privately-held company, Sikka Software is headquartered in San Jose, California with offices in the United States and in India. More information may be found at www.sikkasoftware.com.