The inevitability of neck and back pain
Are you doomed to a life of pain? Not if you take steps now.
By Jeff Carter, DDS
I am unaware of a retired dentist with 30 or more years in practice who has escaped debilitating neck and back pain issues during his or her career. I would also assume many retired practitioners continue to live with accumulated musculoskeletal damage in specific neck and back areas thanks to the stress of awkward dental operator positioning that is seen as essential to delivering quality dental treatment.
How is this possible with decades of advancements in equipment and clinical techniques? Unfortunately, an ergonomic contradiction in dental treatment delivery will exist until equipment configurations, optical/video systems, seating options, or delivery unit configurations are radically altered to allow operators to gain access to the oral cavity while maintaining neutral or balanced posture. In the last 30 years, loupes are the only significant ergonomic supporting device to impact dentistry. With the decreased teaching emphasis on four-handed dentistry techniques and ergonomics in dental schools, neck and back pain issues for all practitioners are equally if not more prevalent than 20 or 30 years ago.
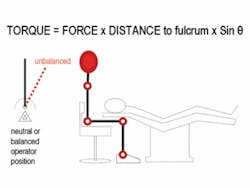
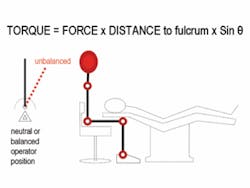
A quick refresher on physics will help objectively define this issue. Most ergonomic injuries in dentistry result from counteracting torque for prolonged periods of time. Torque or “rotational force” occurs when a system becomes unbalanced (image above).
The main culprit in torque generation as it relates to operator position is our own head. The human head is 8 percent of our total body weight. The average man’s head is 14 pounds and the average woman’s head is 11 pounds. For those who participated in diving or gymnastics, you fully understand the influence head weight and head position have on body movements. In the simplest terms, we all have a “bowling ball” affixed to the top of our spine.
In an effort to achieve a direct line of vision into the oral cavity, operators are required to lean or tilt forward in some manner. This is a delivery requirement even when using a mouth mirror and loupes, although both implements can decrease the degree of forward lean or tilt, which is helpful to reduce torque.
Two significant types of operator forward lean or tilt occur commonly in treatment delivery. The first type is often described as head declination with the fulcrum point positioned in the cervical area of the neck (below).
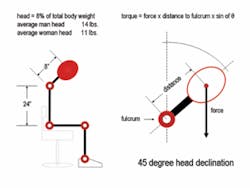
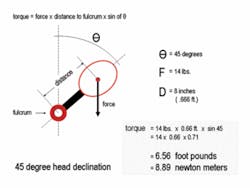
Torque, a rotational force, is measured in foot pounds (or newton meters for you scientific purists). For every second your “bowling ball” head is positioned in a 45 degree forward lean or tilt originating from the cervical area of your neck, 6.56 foot pounds of torque must be resisted to prevent your face from crashing into your chest (below). So what? Consider the following analogy - maintaining your head in this 45-degree forward tilt for 10 minutes requires muscular exertion equivalent to curling a 20-pound dumbbell 92 times!
Torque due to forward head tilt is predominantly resisted by your erector spinae which originate on your sacrum and insert into the occipital notch on the back of your skull.
A second type of operator forward lean or tilt produces an even more dramatic comparison. It is common observe operators leaning forward from the pelvis as much or even more than 30 degrees to gain a more favorable vision line into the oral cavity. In this position, the torque formula distance component is greatly increased (below) and 18.62 foot pounds of torque must be resisted by lumbar region erector spinae.
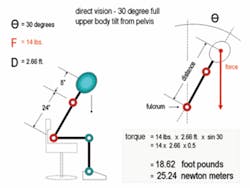
Maintaining your head position in a full upper body lean or tilt of 30 degrees from the pelvis for 10 minutes requires muscular exertion equivalent to curling a 20-pound dumbbell 266 times or curling a 100-pound barbell 53 times!
Weightlifting and resistance training can be great exercise with many physiologic benefits. This is not the case with prolonged static contractions required to maintain common operator positions. In fact, prolonged static contractions of muscle groups (such as the erector spinae in the lumbar and cervical areas) can actually result in diminished blood flow into and out of an area due to compression and lack of dynamic movement. Reduced blood flow and prolonged periods of compression often lead to degeneration of muscle, skeletal, and nerve tissue in the affected areas.
Is it possible to practice dentistry in a neutral or balanced operator position and avoid the damaging health consequences of resisting torque? Not really - unless you can deliver treatment through a surgical microscope which allows you to sit in a neutral balanced position due to an optically repositioned vision line to the oral cavity. Younger endodontists are very proficient in the use of the microscope and will benefit greatly from the healthy positioning ergonomics associated with microscope usage. For the rest of the profession, routine use of a microscope during treatment delivery does not appear to be eminent.
If it is not possible for you to provide quality treatment delivery in a neutral or balanced posture, what can help you minimize the damaging health consequences of prolonged torque resistance?
• Assume a neutral or balanced posture at all times not requiring a direct vision line to the oral cavity. Many opportunities exist during treatment to allow back and neck muscles to relax as you await anesthesia, setting of materials, etc.
• Operator stool selection can help support your specific positioning requirements. The moment you lean forward in your stool and create torque, the entire body is subject to rotational force. Often “perpetual leaners” experience pressure points on the underside of their thighs, resulting in numbness and pain at the pressure point as well as lower leg and foot areas. Operator stools such as those manufactured by RGP and Brewer have a forward tilt built into the seat surface to more evenly distribute force along the hamstring area.
For operators with severe lower back pain, an armrest for the non-dominant hand is a good starting point to allow for a portion of the leaning torque force to be transferred from the lumbar region erector spinae and onto the elbow cup of the stool.
There is no magic stool that will eliminate neck and back strain associated with typical operator positions. It would take an operator stool with a chest pad and a chin rest to transfer the majority of the leaning torque stress currently resisted by neck and back muscles to the stool structure. These stools are in development and create many other side issues yet to be dealt with (as you can imagine).
• Dental patient chair selection is crucial as to how far you must lean to gain an acceptable vision line to the oral cavity. The traditional ironing board back dental patient chairs - such as manufactured by DentalEZ - are best for sliding closer to the patient and minimizing forward lean and tilt. The thicker-backed chairs push the operator farther away from the oral cavity and thus require more forward lean or tilt from the operator resulting in more torque and more muscular exertion. I often recommend the A-dec 500 Series chair as a good combination of thin back for operators and contemporary styling attractive to patients.
• Good operatory design can support and promote healthier ergonomic operator positions. For example, one aspect of good operatory design positions the oral cavity, delivery unit, and all supporting surfaces at the same height above the finished floor. This height is typically 30 to 32 inches and height synchronization creates a working plane that minimizes leaning and tilting movements.
• Exercise and physical therapy should be part of every dentist’s routine. Today’s physical therapy regimens are very sophisticated. You tell the therpaist where it hurts and he or she will design a series of exercises to strengthen and rehabilitate the damaged areas.
Awkward and torque producing operator positions resisted by prolonged static muscle contractions are the main occupational hazard to a dentist’s physical well being. If you were a fireman, this would be your time in the fire - get in there, do your job as professionally and successfully as possible, and then get the heck out of there.
Dr. Jeff Carter is co-owner of the Practice Design Group, based in Austin, Texas. PDG specializes in providing architectural, interior design and equipment, and technology integration services to dentists nationwide. Dr. Carter may be contacted by phone at (512) 295-2224, by e-mail at [email protected], or by visiting PDG’s Web site at www.practicedesigngroup.com.