Eeny, meeny, miny, mo: Dental repercussions from a 25-foot fall

He fell 25 feet while working on a crane, lost consciousness, and underwent cranioplasty surgery for a skull fracture. Furthermore, he had teeth nos. 1, 6, 7, 16, 17, 18, 19, 31, and 32 removed (figure 1). A workers’ compensation claim was filed as the patient understandably wanted his teeth fixed, replaced, and back to the status quo prior to the injury. Seems simple, right? Wrong. Sooooooo wrong.

A healthy 31-year-old male reports that besides a visit to the dentist four years ago to have a bridge done on the upper right side, any previous dental visits occurred when he was around 14–15 years old. Upon initial examination with radiographs (by a previous dentist shortly after the accident), it was determined that the patient had caries on teeth nos. 8, 9, 12, 13, 15, and 30 with advanced, generalized class III periodontal disease. Interestingly enough, it was also determined that the patient was “totally temporarily disabled” for one week following his surgery and extractions. One week.
These options were given to replace the missing teeth:
- Implants on nos. 6, 7, 18, and 19 plus facial resins on nos. 8, 9, and 22 with four quads of scaling and root planing
- Eight-unit PFM bridge from teeth nos. 2–9, crowns on 20 and 21 with a cantilever pontic to replace no. 19, facial resin on no. 22, and four quads of scaling and root planing
- Maxillary and mandibular lower partials, facial resins on nos. 8, 9, and 22, and four quads of scaling and root planing.
Shortly thereafter, the patient moved into my neck of the woods. Enter yours truly. You all know me by now—I’m a tell-it-like-it-is kind of person, and I play by my rules—especially when someone else who has never seen the patient tries to dictate what I will and will not do.
After reading the records sent over by the patient’s previous providers, I did my own examination and noted a few additional things of importance:
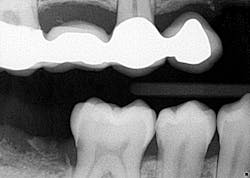
- Teeth nos. 14 and 15 both had supererupted into the 18 and 19 space (figure 2).

- There was positive spacing in the upper right/anterior quadrant, larger than the replacement of teeth nos. 6 and 7 would fill.
- Additional caries were noted on nos. 10, 11, 14, 26, 27, and 29—primarily facial/buccal caries (figures 3–8)





- In the aforementioned treatment plans, nowhere was it noted or discussed what would happen to the caries on the other teeth aside from nos. 8, 9, and 22.
- The patient and his representative (who was present during my exam of the patient) more or less hinted that they wanted me to claim that all of the caries were caused by the fall. Additionally, it was made clear that the patient was unable to personally invest in his teeth at this time. Red flags, people, red flags...
I put an entire treatment plan together that addressed the caries, perio, and replacement of the missing teeth, which included a consult with an oral surgeon. The patient clearly had needs, and I was not going to pick and choose what I would do because he was injured. A cavity is a cavity is a cavity. Everything was submitted to the workers’ comp company. If you have ever done one of these claims, you know that they are a pain in the you-know-what. The paperwork is endless, handwritten, and must be accompanied with all of the necessary documentation to “prove” all findings in order to support subsequent recommendations. More than six months of back and forth. Six months! Something of import to note is that not once did the patient call, inquire, or express concern as to how the case was progressing.
When all was said and done, in a nutshell, the claims company essentially handpicked which teeth they were going to fix, replace, and address. Apparently, in their minds, the caries on no. 8 were caused by the accident, but the caries on no. 9 weren’t. Implants on nos. 18 and 19 were a go, but the supereruption of nos. 14 and 15 didn’t matter and wasn’t their problem. According to the company, the fact that the patient had not had any kind of cleaning for 15 years was clearly irrelevant to his severe periodontal condition, but when you are rendered totally disabled for one week, I suppose that legitimizes the reason he had class III periodontal disease. Hand to forehead! There were a few other things, but you get the point. Are your eyes rolling to the back of your head yet?
So. Frustrating.
At this point I knew this entire case was going south, since it all boiled down to this: How can you selectively look at this patient and pick and choose which caries/oral conditions were a direct result of his injury—i.e., cause and effect? You can’t, unless you have up-to-date previous records on which to base your findings.
I am not beholden to the claims company. As much as I recognized the fact that this patient needed some dental work done, I was not going to piecemeal his care just because somebody behind a desk picks and chooses which fillings were caused by a 25-foot fall. You simply cannot tell me that the genesis for the caries on tooth no. 8 is any different than tooth no. 9. Huge liability factor! I won’t buy it, and I’m not going to play the game.
So, what did I do? I dismissed the case. It wasn’t worth my time, headache, or potential for liability issues to arise. What’s more, the patient really didn’t care, so why should I? It sounds callous, but I have plenty to do without dictating letters and justifying my recommendations to a workers’ comp claims company.
These types of cases can definitely bring to light things that we see as very black-and-white. When issues are financially driven, the debates and arguments for what would normally be simple indeed take a turn, and we have to ask ourselves, “Is it worth it?” Sometimes it is, and sometimes it isn’t. You make the call.
All the best, my friends!
Stacey
Editorial Director, Breakthrough Clinical
Last month: Let’s talk about the ‘D’ word in dentistry
Editor's note: This article originally appeared in Breakthrough Clinical, a clinical specialties newsletter from Dental Economics and DentistryIQ. Read more articles at this link.

About the Author

Stacey L. Gividen, DDS
Stacey L. Gividen, DDS, a graduate of Marquette University School of Dentistry, is in private practice in Montana. She is a guest lecturer at the University of Montana in the Anatomy and Physiology Department. Dr. Gividen has contributed to DentistryIQ, Perio-Implant Advisory, and Dental Economics. You may contact her at [email protected].