Polyphenols and oral health

UV irradiation from the sun and reactive oxygen species (commonly known as free radicals) initiate aging and skin cancer development. Our bodies have natural antioxidant defenses, but free radicals can overcome these defenses and heighten our body’s protective response to the point it causes us harm.
Polyphenols are natural plant compounds, high in antioxidants, that can be absorbed either through our diet or applied directly to the skin to support our natural system. They have also been found to have anticancer, anti-inflammatory, and antimicrobial properties.2
How do polyphenols work?
You may remember from school that we have defense enzymes, such as matrix metalloproteinases (MMPs). One of these is collagenase (MMP-1), but there are other MMPs that have been linked with the progression of periodontal disease, and even cancer. MMPs are active both in the skin and the mouth and are generally beneficial, as they allow removal of damaged proteins.
However, if there is an overexpression of MMPs caused by free radicals, then there is accelerated degradation of collagen, leading to loss of firmness and elasticity of skin. Polyphenols can scavenge free radicals and inactivate MMPs, improving normal skin turnover and health. Not all polyphenols are equal, and tea extract has been shown to have the highest inhibitory activity on both enzymes and antioxidant activity.1
In their review article, Zillich et al. explain that to work on the skin, the active ingredients have to be freely available in the cosmetic formulation and able to penetrate through the outer skin barrier layer called the stratum corneum to reach the epidermis and dermis. Although lab in-vitro studies are very promising, only few clinical studies examining polyphenols have shown an anti-aging effect in human volunteers in-vivo.
Green tea extract is possibly the most studied, and results from topical applications can be varied. One study on 40 women who received green tea therapy as a combination of topical application and oral supplements did show an anti-aging effects when determined histologically.3 Other clinical trials with combined topical applications and oral polyphenol supplements showed benefits with decreased skin roughness and increased skin elasticity and hydration.1
In summary, just because a cosmetic contains active ingredients it is not necessarily going to reach the parts to be effective—as ever, we need to look beyond all the fancy and expensive packaging.
What makes polyphenols exciting for dentistry?
Is there good evidence for polyphenols in our field of interest? Can we use them slow the aging of teeth?
One of our biggest challenges in practice is the care of patients who suffer from root caries. As we age, we are subject to a combination of effects. The recession of gingiva means that the complicated root anatomy involving dentine is exposed. This is far more susceptible to caries than enamel, as demineralization occurs at pH around 6.0, rather than 5.0 for enamel.4
Aging and polypharmacy decrease saliva quality and quantity. Other effects of aging can mean diminished oral hygiene, either through physical infirmity such as arthritis or mental challenges such as dementia. Root caries can progress rapidly, resulting in circumferential lesions that extend subgingivally, which can be almost impossible to restore (figure 1). The two main causes of tooth loss in the older population are periodontitis and root caries.5 Teeth are crucial to our social and psychological well-being, and tooth loss leads to decreased quality of life.4

To understand preventive approaches to root caries and keeping the mouth youthful, it is important to also understand the process of root caries. Dentine is made up of organic substances (mostly collagen) forming a support matrix for the inorganic minerals of calcium and phosphate in apatite. Acid formed by cariogenic bacteria in plaque cause demineralization with the loss of calcium and phosphate ions and exposure of the softened demineralized organic matrix.6
The good news is that at this stage caries is reversible; the ions can return to the exposed matrix and this will avoid the complexities and costs of a tooth restoration. However, collagenase and other MMP enzymes produced by bacteria and inherent within our own saliva and dentine are activated by the acidic conditions and break down the collagen scaffold, making remineralization impossible.6
Researchers at the Dental School of University of Illinois have investigated oral care strategies with the aim of (1) diminishing the cariogenic bacteria that cause root caries, (2) neutralizing the acidic conditions, (3) preventing the collagen scaffold breakdown, and (4) allowing calcium and phosphate remineralization. The conceptual approach of this was to use xylitol, green tea extract polyphenols, and amorphous calcium phosphate.7
An almost unprecedented study into the effects of xylitol in adults was reported in 2013.8 The study looked at 691 people in the United States, comparing peppermint xylitol lozenges with control (nonsugar) lozenges over 33 months. It was a multicenter, placebo-controlled, double-blind, randomized-control clinical trial. When the data were analysed by looking at site-specific caries, there was a significant benefit in using xylitol in root caries: “Participants in the xylitol arm developed 40% fewer root caries lesions than those in the placebo arm.”9
Of particular significance in the xylitol study8,9 is that the participants lived in areas with fluoridated water and regularly used fluoride toothpaste, so the xylitol benefit was in addition to their routine oral hygiene. Xylitol has been recommended to augment the control and maintenance of root caries within the minimum intervention dentistry approach.10
More recently, calcium phosphate supplementation has been advocated to help with remineralization and neutralization of acids in such products as MI Paste Plus (GC America; also known as Tooth Mousse in Europe). However, at near-neutral resting pH, the saliva is naturally supersaturated with calcium and phosphate ions in readily bio-available salivary proteins.11 Therefore the greatest benefit of supplementation of these ions would be in a population with reduced saliva, such as the approximately 30% of those over 65 years of age who suffer from xerostomia.12,13
Polyphenols in dentistry have been widely investigated for their potential to improve dentine remineralization, dentine strength, and bonding to restorative materials, and also for their natural antimicrobial compounds as an alternative to common chemicals for caries prevention. The two main sources are green tea extract and grape seed extract.6 The component of green tea extract that has been found particularly valuable in dental research is epigallocatechin gallate (EGCG). EGCG has been shown to reduce the biofilm formation of Streptococcus mutans, acting as a natural antimicrobial agent, as well as improving the mechanical properties of dentine.14
However, the inclusion of green tea extract is not necessarily adequate to allow remineralization or to be effective in plaque neutralization.7,15 Other studies have compared solutions of EGCG, chlorhexidine, and stannous fluoride, and found all of these enzyme inhibitors reduced dentine wear significantly, but suggested that using a rinse after every acidic challenge to be impractical.16
A novel home-care product
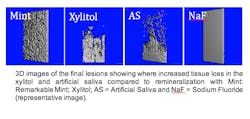
The novel mint product (Dr. Heff’s Remarkable Mints) researched by the Dental School at University of Illinois was invented by UK dentists as a way to overcome the challenges of daily dental care for busy patients. The patent-pending formulation includes green tea polyphenols (EGCG) to maintain the collagen scaffold, xylitol to act as an antibacterial agent, and calcium phosphate. The study showed xylitol alone did not remineralize artificial root caries, as its anticariogenic mechanism is inhibitive of the plaque biofilm. However, the combination of ingredients that are found in Dr Heff’s Remarkable Mints, with the higher concentration of EGCG, showed significant remineralization due to maintaining a crosslinked collagen scaffold for mineral uptake despite acidic and enzyme challenges (figure 2).7
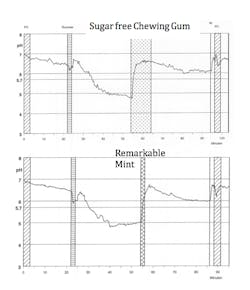
Further research on Dr. Heff’s Remarkable Mints havs been carried out with an in-vivo trial using a micro-electrode inserted into thick plaque of volunteers.17 A sucrose challenge was performed, and a comparison of sugar-free chewing gum and Dr. Heff’s Remarkable Mints showed very similar immediate rates of acid neutralization. Previous in-vivo studies have also shown the benefits of EGCG in neutralizing acid in cariogenic plaque following sucrose solutions in volunteers15 and reduction in plaque formation in-vivo.18
Research by Toothfriendly International at University of Zurich17 highlights the beneficial effects of neutralizing acid and penetration within the biofilm (figure 3).7 This extent of research on a dental mint is unusual. For further information, visit drheffs.com.
Conclusion
The polyphenols included in Dr Heff’s Remarkable Mints are an excellent, convenient adjunct to regular oral hygiene measures with fluoride toothpaste, particularly in patients that are higher risk of caries and erosion.
References
- Zillich OV, Schweiggert-Weisz U, Eisner P, Kerscher M. Polyphenols as active ingredients for cosmetic products. International Journal of Cosmetic Science 2015; 37: 455-464
- Zhao W, Xie Q, Bedran-Russo AK, Pan S, Ling J, Wu CD. The preventive effect of grape seed extract on artificial enamel caries progression in a microbial biofilm-induced caries model. J Dent 2014; 42:1010–1018.
- Chiu, A.E., Chan, J.L., Kern, D.G., Kohler, S., Rehmus, W.E. and Kimball, A.B. Double-blinded, placebo-controlled trial of green tea extracts in the clinical and histologic appearance of photoaging skin. Dermatol.-Surg. 2005; 31: 855–859.
- MacEntee MI, Bryant SR, Keller H et al. Caries control for frail elders. In: Dental caries: The disease and its clinical management, 3rd Edn. Fejerskov O, Nyvad B, Kidd E, (eds). Oxford,:Wiley Blackwell 2015 321- 32.
- Gati D, Vieira AR. Elderly at greater risk for root caries: A look at the multifactorial risks with emphasis on genetic susceptibility. Int J Dent. 2011: Articles ID 647168, 6 pages, 2011. doi:10.1155/2011/647168.
- Bedran-Russo AK, Pauli GF, Chen AN et al. Dentin biomodification: strategies, renewable resources and clinical applications. Dent Mat. 2014; 30(1): 62-76
- Zamperini CA, Bedran-Russo AK. Remineralization potential of mints containing bioactive agents in artificially induced root caries. Caries Res. 2018; 52: 331-338
- Bader JD, Vollmer WM, Shugars DA Gilbert GH, Amaechi BT, Brown JP, Laws RL, Funkhouser KA, Makhija SK, Ritter AV, Leo MC. Results from the Xylitol for Adult Caries Trial (X-ACT). J Am Dent Assoc. 2013; 144 (1): 21- 30.
- Ritter AV, Bader JD, Leo MC, Preisser JS, Shugars DA, Vollmer WM, Amaechi BT, Holland JC. Tooth-surface-specific effects of xylitol: randomized trial results. J Dent Res. 2013; 92 (6): 512-7
- MI Dentistry Handbook, A comprehensive guide to treatment plans and practice implementation of minimum intervention dentistry. GC Corp 2017.
- Ten Cate JM, Larsen MJ, Pearce EIF. Chemical interactions between the tooth and oral fluids. In: Dental caries. Fejerskov O, Kidd EAM, editors. Oxford, UK: Blackwell Munksgaard 2004: 49-69
- Ship J, Pillemer S, Baum BJ. Xerostomia and the geriatric patient. J Am Geriatr Soc. 2002; 50 (3): 535-43.
- Cochrane NJ, Reynolds EC.Calciumphosphopeptides- mechanisms of action and evidence for clinical efficacy. Adv Dent Res. 2012; 24 (2): 41- 47
- Xu X, Zhou XD, Wu CD. Tea catechin epigallocatechin gallate inhibits Streptococcus mutans biofilm formation by suppressing gtf genes. Archives of Oral Biology 2012; 57: 678–83
- Hirasawa M, Takada K, Otake S. Inhibition of Acid Production in Dental Plaque Bacteria by Green Tea Catechins. Caries Res. 2006; 40: 265-270
- Magalhes AC, Wiegand A, Rios D, Hannas A, Attin T, Buzalaf MA. Chlorhexidine and green tea extract reduce dentin erosion and abrasion in situ. J Dent. 2009; 37: 994-998
- Unpublished Data: Toothfriendly International, Department of Periodontology, University of Zurich 2016
- International Journal of Innovation and Scientific Research ISSN 2351-8014 Vol. 16 No. 1 Jun. 2015, pp. 171-178 The effect of green tea mouthrinse in a 4 day plaque regrowth model in vivo and antibacterial efficacy in vitro: a randomized controlled trial.
Michael Heffernan, MS, BDS, graduated from Guy’s Hospital (UK) and completed his master’s degree in prosthodontics at the University of Iowa. His research won the prestigious John J. Sharry Research Prize from the American College of Prosthodontists. He was awarded an implant scholarship at the University of Florida. He returned to the UK and works clinically as a specialist prosthodontist. He lectures internationally, writes regular dental articles for The Daily Telegraph, and is cofounder Dr Heff’s Remarkable Mints.
About the Author

Michael Heffernan, BDS, MS
Michael Heffernan, BDS, MS, graduated from Guy’s Hospital (UK) and completed his master’s degree in prosthodontics at the University of Iowa. His research won the prestigious John J. Sharry Research Prize from the American College of Prosthodontists. He was awarded a scholarship at the University of Florida in a dedicated implant fellowship. He practices in the UK, is a clinical lecturer at the Eastman Dental Institute (UCL), and cofounded Dr. Heff’s Remarkable Mints. For more information, email [email protected].
Updated June 13, 2023