Classifying occlusion: Board exam tips from StudentRDH.com

ByClaire Jeong, BS, MS, RDH, and Delphine Jeong, DMD
Occlusion is defined as the contact relationship of the maxillary and mandibular teeth when the mouth is fully closed. Occlusion is important because it can influence a person’s facial profile and also the health of the oral cavity. Occlusions that are not ideal may be improved with dental treatments such as orthodontics. In this article, we are going to examine some of the most fundamental concepts that dental professionals need to know when classifying occlusion.
Understanding perfectly those concepts will not only help you score more points in the dental hygiene board exams but will also make you a stellar clinician that everyone would want to work with!
1. Overjet and Overbite1
If you look at the human skull, the maxilla is larger than the mandible. This anatomy makes the maxillary arch larger than the mandibular arch and in turn creates a natural overjet/overbite that we will discuss in this section.
Overjet: In professional terms, it is the horizontal overlap of the maxillary central incisors over the mandibular central incisors. In simple terms, it is how much the upper front teeth protrude forward in relation to the lower front teeth. The amount of overjet is measured using the probe horizontally. The normal overjet is considered to be 2-3 mm. Here is a tip to help you remember overjet: jets fly horizontally.
Overbite: In professional terms, it is the vertical overlap of the maxillary central incisors over the mandibular central incisors. In simple term, it is how much the upper front teeth cover the lower front teeth in a vertical dimension. The amount of overbite is measured using the probe vertically. The normal overbite is considered to be 2-3 mm, or approximately 20–30% of the height of the mandibular incisors.
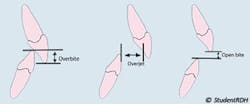
Sometimes, the maxillary teeth do NOT overlap the mandibular incisors in a vertical or horizontal dimension. Edge to edge (end to end) relationship (upper and lower anterior teeth meet in a straight line, no overjet, no overbite) and open bite (no overbite, often associated with tongue thrust) fit into those cases.
2. Angle’s Classifications of Occlusion2
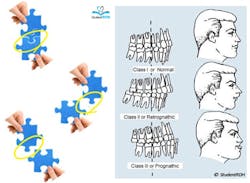
In the early 1900s, Edward H. Angle classified occlusions using the relationship between the first molars of both arches as the key factor in determining occlusions. The three classes according to Angle’s classification are as follows:
- Normal occlusion: The mesiobuccal cusp of the upper first molar occludes with the buccal groove of the lower first molar.
- Class I malocclusion: Same as normal occlusion but characterized by crowding, rotations, and other positional irregularities.
- Class II malocclusion: The mesiobuccal cusp of the upper first molar occludes anterior to the buccal groove of the lower first molar. There are two subtypes of Class II malocclusion.
- Class II, division 1: Upper incisors are tilted outwards, creating significant overjet.
- Class II, division 2: Upper incisors are labially inclined.
- Class III malocclusion: The mesiobuccal cusp of the upper first molar occludes posterior to the buccal groove of the lower first molar.
Recreated images of puzzle pieces are used below to illustrate the relationships between the first molars. Imagine the protruded part of the top puzzle piece (representing the mesiobuccal cusp of the upper first molar) fitting into the indent of the bottom piece (representing the buccal groove of the lower first molar). Now move the top piece “forward” to create Class II malocclusion or move it “backward” to create Class III malocclusion.
Review the example below.
Q: According to Angle’s classifications of occlusion, the patient has:
A. Normal occlusion
B. Class I malocclusion
C. Class II malocclusion
D. Class III malocclusion
Answer: C. Class II malocclusion
To solve the question, first identify the mesiobuccal cusp of the maxillary first molar and see if it fits in the mesiobuccal groove of the mandibular first molar. In this case, the mesiobuccal cusp of the maxillary first molar is “anterior” to the groove of the mandibular first molar. Therefore, we can conclude that the patient has Class II malocclusion. Class II malocclusion can be further divided into Division 1 or Division 2, but this cannot be determined since the anterior teeth are not presented in the case.
Now that we have learned the basic concepts related to occlusion, take the time to master them. They are extremely important fundamental information and are likely to be emphasized in the dental hygiene board examinations.
Claire Jeong, BS, MS, RDH, is the founder of StudentRDH, a review solution for the National Dental Hygiene Board Exams and Dental Hygiene Local Anesthesia Exams. She graduated from MCPHS University, Forsyth School of Dental Hygiene; served as a student delegate for the ADHA; and is a member of Sigma Phi Alpha, the dental hygiene honor society. Claire is committed to improve dental hygiene education and help students from all around the country pass their board examinations. Claire is licensed in the United States and Canada. She provides personalized mentorship at StudentRDH and can be reached at [email protected].
Delphine Jeong, DMD,is the co-founder of StudentRDH, a review solution for the National Dental Hygiene Board Exams. She received her doctor’s degree from Boston University Goldman School of Dental Medicine and her Bachelor’s degree from Purdue University. She has a great passion for community health and cultural literacy. Dr. Jeong is licensed in the United States and Canada.
References
- Darby ML, Walsh M. Dental Hygiene: Theory and Practice. 4th ed. St. Louis, MO: Elsevier Saunders; 2015.
- Rashid EG. Operative Dentistry. In: Scheid RC. Woelfel’s Dental Anatomy. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007.