Not on my watch!
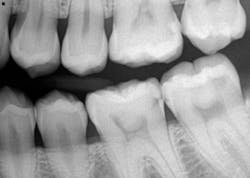
A 26-YEAR-OLD FEMALE PRESENTS for a new-patient exam. She had already been seen for a limited exam and subsequent extraction of a wisdom tooth. She was diagnosed with generalized Class II periodontal disease and multiple restorative needs, including gross apple-core and interproximal caries. It is highly likely that several teeth will end up needing crowns and possible root canals. However, due to the extent of perio, the immediate goal is to stabilize and arrest the caries. Restoring form and function will soon follow. See Figures 1 and 2.
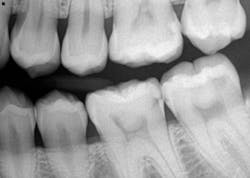

The patient came in for two fillings, both of which were quite deep and may have caused irreversible damage. She then disappeared for nine months, and when she returned, wouldn’t you know it—one of those teeth needed a root canal. Oh, and by the way: “I’ve been doing Invisalign for the last six months. Will this affect the fit of the aligners?”
Wait. Just. One. Minute.
I took a generalized glance in her mouth and, yup, gross caries was everywhere. Still. And the patient is in Invisalign aligners. That dark tooth in the front didn’t just get there for no reason.
I informed the patient that the root canal itself wouldn’t affect the fit of her upper aligner; however, I bluntly stated that I was concerned she was even in aligners! Furthermore, I was going to contact the orthodontist and advise him to cease Invisalign treatment until the restorative needs were taken care of.
But wait—it gets better. “Can you please not tell the orthodontist to stop my care, because I only have a few trays left?”
There are three things that come to mind with this case:
1. This is the kind of stuff the DIY ortho cases are all about. Get your teeth straight, but don’t worry about the filling, crown, or root canal you might need. Not to mention the periodontal issues! Oral health? What’s that?
2. Is this supervised neglect? The progression of the aligners was done under the care and license of an orthodontist. The patient was clearly aware at her initial visit—from both me and the orthodontist—that she needed to get the dental work done. But she didn’t.
3. What should ultimately transpire? Who has the badge of control here—the patient, the orthodontist, or me?
Let’s be clear. I enjoy good working relationships with all of the specialists to whom I refer. My patients are in good hands while in their care. However, sometimes what patients say and actually do are two different things, and what they tell one doctor may be completely different than what they tell another. Be that as it may, according to the orthodontist, the patient was getting her work done, although in baby steps and a one-filling-at-a-time scenario. Since she had an entire mouthful of work that needed to be done, the orthodontist’s trust in the patient had no reason to be invalidated. Time ticked away, and movement was being made with the patient’s teeth. Caries was not being addressed though. Not even for one tooth.
My discussion with the orthodontist was to the point. Treatment needed to stop until the patient was cleared to commence with aligners. Plain and simple. It boils down to liability and what we, as professionals, are going to allow to happen under our watch. The orthodontist readily agreed, and ortho treatment has ceased.
It is not our job to hold our patients’ hands and force them to establish and maintain oral health. But it is our job to take charge of situations that are in our control and set boundaries within the patient/doctor relationship.
Don’t let your patients dictate how you provide care. This goes back to the blog I wrote a couple months ago about the patient who refused radiographs. I gave that patient the option either to leave or allow me to do my job. Trust and motivation are gained by lending your ear to patients’ concerns, educating them, and drawing the line on what you will or will not do in their best interests. Now, I’m not saying there can never be a compromise, but be willing to stand your ground! In this particular case, those carious teeth were (and still are) a huge issue, and I’ll be damned if the patient is going to simply maintain the status quo on my watch.
The emphasis of outward esthetics in an individual is rather driven in our world of social media, so much so that sometimes little consideration is given to overall health—and in this case, oral health. We see this type of situation with whitening cases and now, sadly, the DIY ortho victims.
In this case, the orthodontist and I were able to stand together and paint a scenario that in the end was much more appealing to the patient. No matter how many aligners she puts in her mouth, that dark tooth in the front won’t go away on its own, and, in fact, it will supersede the beauty of her straight teeth every single time she smiles.
What’s the take-home?
Work with your referring doctors. Build trust and open lines of communication so that when there is a concern, you won’t have to dance around the issue because you’re concerned about hurting feelings. This is business, and we have a job to do. There’s no time for emotional roller coasters and tiptoeing around conversations.
Love what you do and learn along the way for the betterment of yourself, the profession, and our patient care.
Cheers, my friends!
Stacey
Stacey L. Gividen, DDS
Editorial Director, Breakthrough Clinical
LAST MONTH >> She had trained herself not to smile
Read more clinical dentistry articles at this link.
Editor's note: This article originally appeared in Breakthrough Clinical, a clinical specialties newsletter from Dental Economics and DentistryIQ.

About the Author

Stacey L. Gividen, DDS
Stacey L. Gividen, DDS, a graduate of Marquette University School of Dentistry, is in private practice in Montana. She is a guest lecturer at the University of Montana in the Anatomy and Physiology Department. Dr. Gividen has contributed to DentistryIQ, Perio-Implant Advisory, and Dental Economics. You may contact her at [email protected].