Restore that posterior tooth ... directly

By Christopher Ramsey, DMD
Articles detailing the benefits of posterior composites and the most effective placement techniques to ensure clinical and esthetic success are plentiful throughout dental literature. Unfortunately, in almost all cases, such articles reiterate a practical observation that is quickly becoming invalid — treatment with direct posterior composites is time-consuming and overly technique-sensitive.
As a result, there are many (but certainly not all) dental professionals — even those who practice "esthetic dentistry" — who are unwilling to provide the ultimate in direct posterior restorations. To justify their reluctance to placing such restorations, some practitioners will counsel patients that composite fillings don't work, or that only opera singers need to have white fillings. Possibly worse yet, there are some dentists who provide posterior composite fillings that press one piece of B1 material into the preparation with their thumbs, grind in the occlusion, and then send the patients on their way.
Such aversion to, and hurried placement of, direct posterior composites is unnecessary. Today's dental products and technology can help make anything possible, including long-lasting, easily placed, and natural-looking posterior fillings. 1-4 In fact, today's materials and instrumentation offer dentists the most simple, cost-effective, and immediate manner in which patients are provided with clinically sound, functional, durable, and esthetic treatments in the posterior of the mouth.
Clearly, however, there are dental professionals doubtful of the truth behind this assertion and in need of a timed session to determine if placing direct posterior composite restorations is worth the time and effort. Therefore, this article presents a step-by-step, minute-by-minute account that reveals how long it actually takes to provide a high-quality posterior occlusal composite restoration.
A case in point
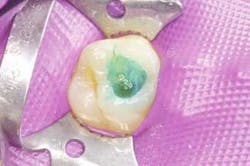
A 24-year-old female patient presented with caries on tooth #3. The decay present in the mesial half of the tooth was of adequate size for restoration with a direct posterior composite.
null

null

null

null

null

null

null

null

null

null

null
Conclusion
The posterior occlusal composite restoration presented was completed on tooth #3 in 27 minutes. At a time when today's restorative materials fulfill basic treatment requirements and simultaneously achieve a natural-looking blend with a patient's natural teeth, 27 minutes is not too much time to spend in order to provide a superior restoration. As a result of enhancements to material handling, esthetics, and wear properties, today's direct posterior dental composites can be used quickly and easily to satisfy treatment demands. And, with the variety of highly acclaimed hands-on training seminars offered throughout the country, clinicians can now use their thumbs as fingers, not as condensers.
Note: References available upon request.
Dr. Christopher Ramsey practices esthetic restorative dentistry at the Studio of Esthetic Dentistry in Palm Beach Gardens, Fla. Dr. Ramsey is currently an instructor at the Institute for Oral Art and Design in Bradenton, Fla. He can be reached at (561) 626-6667.