A New Dimension in Technology ...CEREC CAD/CAM System

One woman dentist's story about incorporating the newest CEREC CAD/CAM system into her practice ...
Smart women dentists know that the purchase of technology alone will not yield improved productivity or an automatic cash flow. They also know that technology continues to improve over time, and the latest models are often better. It has been my experience that the ongoing effort of integrating technology into our practices helps us obtain our long-term practice goals. I believe that the CEREC System (Sirona) offers patients the best possible dentistry. This is the story about why I decided to incorporate the newest CEREC 3D CAD/CAM into my practice and what that means for me and my patients.
Experience is a great teacher. In 1989, I had five CEREC 1 CAD/CAM restorations placed in my mouth as part of a clinical trial at the University of North Carolina. The untreated caries in my mouth fit the new technology protocol. I was also involved in a second study involving composite material. Due to the quick onset of postoperative sensitivity, I asked that the composite be removed and replaced with a CEREC restoration. Today, all five restorations are still intact and look great. My patients understand that I am recommending the best for them because that is what I demanded for myself. (Figure 1)

Full integration of technology relies heavily on a broad-based approach to team training, as well as clinical protocols such as proper patient positioning and utilization of that technology, where possible, to maximize results. Efficient scheduling is also optimized. In my practice, I recognize that it is my team who ultimately delivers results; technology is merely a tool to increase profitability and productivity, as well as improve the patient's options for cosmetic, highly aesthetic restorations.

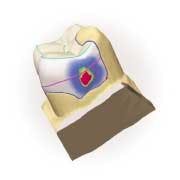
One such technological tool we have found helpful is a CEREC 3D CAD/CAM chairside model, which enables the dental team to complete a preparation and restoration in a single visit. (Figure 2) While some of my colleagues have joked that the best function of some previous chairside CAD/CAM systems was as an operatory coat rack, today's CEREC CAD/CAM systems truly do increase efficiency in my office.
Relying on the support staff
I believe that changing to keep pace with advancements in dental practice is the key to success. It certainly is the key to my success! Ensuring that the entire team is included in these changes makes the integration of technology seamless. It's very important in the early stages to educate your team on what CEREC is before you try to implement this technology. My team members were so enthusiastic about incorporating the system into our practice that many of them who needed restorations opted for CEREC right away. In turn, they can use their own experiences to discuss this new restorative option with patients.

Here's how we use the CEREC CAD/CAM system in my dental practice. The system allows team members, including the dental assistant or hygienist, to help in the restoration design. (Figure 3)1 The system performs a customized milling process based on computer images. Our patients often watch this process. In the states where auxillaries can do certain in-mouth procedures, team members can be fully involved in single-visit dentistry to enhance patient comfort and improve practice efficiency. My team began to share my enthusiasm once they became familiar with the quality of the restorations.
In my practice, dental assistants are allowed to do expanded functions. They perform the powdering and optical imaging, program the computer, and complete the initial try-in.2 As a team, we have developed a clinical plan to which we adhere. This frees me to see other patients while my team facilitates the initial restorative process. While there are many possible approaches, this timing has proved successful for my scheduling purposes:
- Prep: 10 minutes (dentist)
- Powder: 30 seconds (dental assistant)
- Image: 30 seconds (dental assistant)
- Design: 10 minutes (dental assistant)
- Milling: 16 minutes (machine; patient may watch if desired)
- Try-In: 10 minutes (dental assistant)
- Seating: 2 minutes (dentist)
- Finishing/Polishing: 15 minutes (dentist)
⇒ Total: Dentist: 27 minutes + Dental Assistant: 21 minutes + Machine: 16 minutes = 64 minutes from prep to polish!
Proper training and planned implementation for every team member has helped us achieve maximum results in our practice. As with any new equipment, there is a short learning curve; however, after a one-to-two-day basic training seminar, we could use the system shortly after it was installed. We also included the dental assistant and other designated team members at every step in the training process so that integration became as easy as implementation. Our philosophy is that this is a team effort from the beginning of the process to full integration into the practice. Unlike the previous 2-dimensional CAD/CAM software, the new 3-dimensional platform allowed me to learn the system concurrently with my team. Now they have an investment in making it work for the practice.

The options offered in the new software allow me to view the restoration completely in the patient's mouth. I can virtually follow standard lab processes to make a ceramic restoration without the timing, input, and expenses of a conventional off-site lab. Instead, a virtual lab is right there for me, where I can trim my die, inspect and mark my margins, and design my restoration. Then I can immediately convert the designed restoration into the final milled product, all at chairside. (Figures 4 and 5)
Educating the patient
As with any oral health restoration, patient self-care is even more important than the in-office procedures. With self-care, we know that CEREC CAD/CAM restorations will last a long time.3,4,5,6 The aesthetic quality of the materials has been well-documented and reported to have the least postoperative sensitivity of all restorations.7,8 How can we communicate this to patients without boring them with statistical charts and data? We use co-diagnosis because, ultimately, it's the patient's decision; we simply provide the options.
In my practice, we offer amalgam, composite, and CEREC restorations, discussing the advantages of each. Team members describe how the new technology helps retain maximum tooth structure and why that's important to the strength of the tooth. Other advantages we share are one-visit restorations, no impressions, no temporaries, a customized fit, and a final result in an aesthetically pleasing, tooth-colored material. In the end, our patients choose to have the CAD/CAM restorations. Educational tools on CDs (CAESY Patient Education Systems) help patients further visualize dental procedures.
Conclusion
My patients appreciate the one-visit convenience that the CEREC System affords, and it's easy to communicate the advantages to them. But an even greater benefit is the conservative preparation. We know that we can conserve tooth structure with this new technology-aided process, and my patients enjoy being part of it. Involving the patient is the key to success. The CEREC technology has come so far, and with 3D, it's easier than ever. Try it for yourself!
References
- Flucke J. CEREC and the dental assistant. Dental Equipment & Materials 7.3:62-63.
- Morin M. CEREC: the power of technology. Compendium 22(6) (Suppl):27-29.
- Christensen R, Christensen G, Vogel S, et al. Two-year clinical comparison of six inlay systems. J Dent Res 1991; 70:561.
- Isenburg BP, Essig ME, Leinfelder KF. Three-year clinical evaluation of CAD/CAM restorations. J Esthet Dent 1992; 4(5):173-176.
- Reis B. CEREC practice integration. In Mörmann W. CAD/CAM in Aesthetic Dentistry, Quintessence 1996; 267.
- Reis B, Walther W. Clinical long-term results and 10-year Kaplan-Meier estimation of computer-aided machined CEREC-restorations. Int J Comp Dent 2000; 3:20.
- Masek R. Achieving high-level esthetics with CEREC. Compendium 22(6) (Suppl):19-26.
- CRA Report 1999; 23(11).

Julie Spaniel, DDS
Dr. Spaniel graduated from the University of North Carolina at Chapel Hill in 1991 where she was involved as a student in the initial research conducted on the CEREC 1 by Dr. Herald Heyman. She has been in private practice in Burlington, Vt., for the past 10 years. Contact her at [email protected].