Confidence in caries detection

Innovations in technology have given clinicians more tools to diagnose more specifically and consistently. I personally have implemented digital x-rays and an oral cancer screening device. Any new technology, in my opinion, should be added to a practice based on how much the patient will benefit.
When it comes to my diagnostic process, caries detection is an important addition for comprehensive imaging. While digital x-rays are still necessary for other reasons, being able to offer a caries detection method without exposing the patient to radiation gives both me and the patient an extremely accurate second opinion.
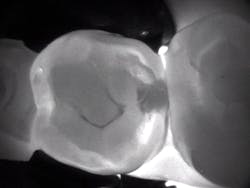
I have used several methods of caries detection, but as technology evolves, I am always looking for something better. My last device used numbers to calculate caries, but I found them to be inconsistent. I did not have a photo of the tooth to keep in the patient’s record. Images from CariVu (DEXIS) look similar to a radiograph, so I can see for myself the dark areas that denote the presence of caries occlusally and interproximally, as well as cracks.
I am fortunate to have monitors in all treatment rooms, and when I use any of my digital imaging technologies, my patients can see their teeth in an image that they can visually understand. For new and existing patients alike, this creates a “wow” factor. During my comprehensive exam, almost all of my patients have made positive comments such as, “This is awesome; I’ve never seen that before.” They notice that my equipment is different from other offices, and it lifts their perception of my practice to a higher level. They don’t question my diagnosis of caries, because they see it too.
Now, rather than just treating caries, I can help to prevent its spread. In some instances, a smaller amount of decay would not be detected by digital x-rays. If the patient doesn’t return for a couple of years, and I miss that early decay, it could easily lead to more invasive treatment. This is when my caries detector is most helpful. When patients see their own caries on the monitor, they are more apt to want me to take action sooner rather than later. They take ownership of their dental care because of this visual aid. After I open up the tooth, I can even use an intraoral camera to show the patient the decalcified or carious area. Even on small caries, CariVu is very predictable with a 99% accuracy rate.1
On the other hand, patients appreciate when my technology can actually lead me to wait instead of treating. In some cases, the CariVu images show a decalcified area that is not full-blown caries yet; that is, not fully into the dentin, but it is in the first stage of decay—even before it appears on a radiograph.2 With this type of incipient caries, sometimes I want to wait and monitor the area. It is interesting to note that after seeing the image, some patients will choose to wait. Others won’t want to wait; they will ask me to move ahead with the restoration.
When an x-ray or visual exam shows what appears to be caries, but the CariVu image does not, I go with CariVu. For example, fracture lines can actually appear as dark-line caries but can also be severe staining. When I maneuver the tip in different angles, sometimes I can actually see this supposed “cavity” disappear. Patients appreciate when I can tell them that the area is not carious. Dentists are trusted, and I want to keep that trust. I don’t want to drill a tooth that may not have decay. All of us dentists have seen what we thought was a cavity on an x-ray, drilled the tooth, and then thought, “Where’s the cavity?” That is an uncomfortable situation that I can now avoid.
Of course patients who are pregnant, those who have had other medical issues that preclude their having more x-rays, or patients who are simply x-ray-reluctant are happy to have this diagnostic option. This is true for any caries detection device. Due to its high accuracy rate, more often than not I choose CariVu, rather than x-rays, for exams on younger children (especially when looking for interproximal caries) because of their sensitive gag reflexes and the small size of their mouths. Recently, I diagnosed three two-surface lesions with a CariVu image on a child with a severe gag reflex, and I was able to treat the child.
The caries detection device is easy to add into the dental office workflow. I use it on every new patient’s comprehensive evaluation. On recare patients, if the hygienist sees a suspicious area in the mouth or on the x-ray, she will quickly take a CariVu image and call me in to see the area of concern. I only have one in the office now, but in the future, each of my hygienists will have this system and use it routinely on every recall visit. This can help us out time-wise, since hygienists can take the pictures quickly, save them, and I can see the images immediately when I walk into the treatment room. While only my assistant and I received initial training on the device, it is very easy to use and was easily explained to our hygiene staff. We began using it the first day.
Besides providing great diagnostic information, the return on investment (ROI) is phenomenal. Overall, as a result of using caries detection, I have probably placed more resin restorations in the past one-and-a-half years than in the last 10. Because of my capacity for earlier and more accurate caries diagnosis and the increase in resins, I paid off my CariVu system in the first three months of owning it. Not only for established dentists, I believe that this ROI makes the system a must-have investment as start-up equipment for any new practice.
Granted, technology makes life easier for the dentist and treatment team; in the computer age, we can process information faster and navigate through procedures faster. But speed is secondary to providing the best dental care possible to our patients. When I am evaluating whether to treat caries sooner or to wait a bit, this next-generation transillumination caries detector keeps me from being in the dark about my patients’ caries.
Disclosure: Dr. Joseph Favia has no financial interest in DEXIS, LLC.
References
1. Kühnisch J. Benefits of the DIAGNOcam Procedure for the Detection and Diagnosis of Caries [study project]. Munich: Ludwig Maximilian University of Munich; 2013.
2. Söchtig F, Hickel R, Kühnisch J. Caries Detection and Diagnostics With Near-Infrared Light Transillumination: Clinical Experiences. Quintessence Int. 2014; 45(6):531–538. doi: 10.3290/j.qi.a31533.

Joseph A. Favia, DDS, is a graduate of Loyola University School of Dentistry. He has taken advanced dental education from the Dawson Academy, the Pankey Institute, and an advanced bone grafting mentorship with Dr. Joel Rosenlicht. Dr. Favia founded the Midwest Surgical Institute for Dental Implants and teaches implant surgical procedures internationally. He maintains a private practice in Arlington Heights, Illinois. You can contact him by e-mail at [email protected].